Introduction
The healthcare sector is large, employing around 11% of workers in the European Union[1]. Employment in the healthcare sector (Nace Q86) increased by 20% between 2008 and 2023 compared to only 5% increase in total employment[1]. Hospitals are the primary employer of healthcare workers, while other employers include medical practices, nursing and care homes and other healthcare activities such as homecare services[2]. The evidence indicates that mental health issues are of increasing concern in the healthcare sector and a number of initiatives have been implemented to address these issues. This article provides an overview of the factors which pose a threat to the mental health of workers in the sector and identifies and evaluates interventions used for promoting the mental health of healthcare workers.
Mental health in the healthcare sector
While exposure to factors affecting mental health substantially varies across all economic sectors, exposure occurred most often in the sector ‘human health and social work activities’ with 58,5% of the workers in the sector reporting to risk factors affecting their mental health[3]. Mental health is described by the World Health Organization[4] as ‘a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’. In this positive sense, mental health is the foundation for well-being and effective functioning for an individual and for a community. Mental health and mental illnesses are determined by multiple and interacting social and psychological factors, including psychosocial hazards, which are prevalent in all workplaces. Psychosocial risks refer to the likelihood that work-related psychosocial hazards will have a negative impact on employees’ health and safety through their perceptions and experience[5].
Psychosocial risk factors
Many work-related psychosocial hazards exist. Those which are typical for the health care sector[6] [7] include amongst others:
Prevalence and incidence of psychosocial risks
Data from the European Working Conditions Telephone Survey (EWCTS 2021) indicate that half of health and social care workers are in "strained jobs" according to the Job Quality Index[8]. This index assesses job quality by comparing the number of demands and resources associated with a job, incorporating indicators from six key dimensions: physical and social environment, job tasks, organisational characteristics, working time arrangements, job prospects and intrinsic job features. Job quality is determined by the difference between the number of job resources and job demands. A job is considered as "strained" when demands exceed resources, while it is considered "resourced" when resources outweigh demands[9].
Figure 1: Job quality index, by worker group, EU - EWCTS 2021 (%)
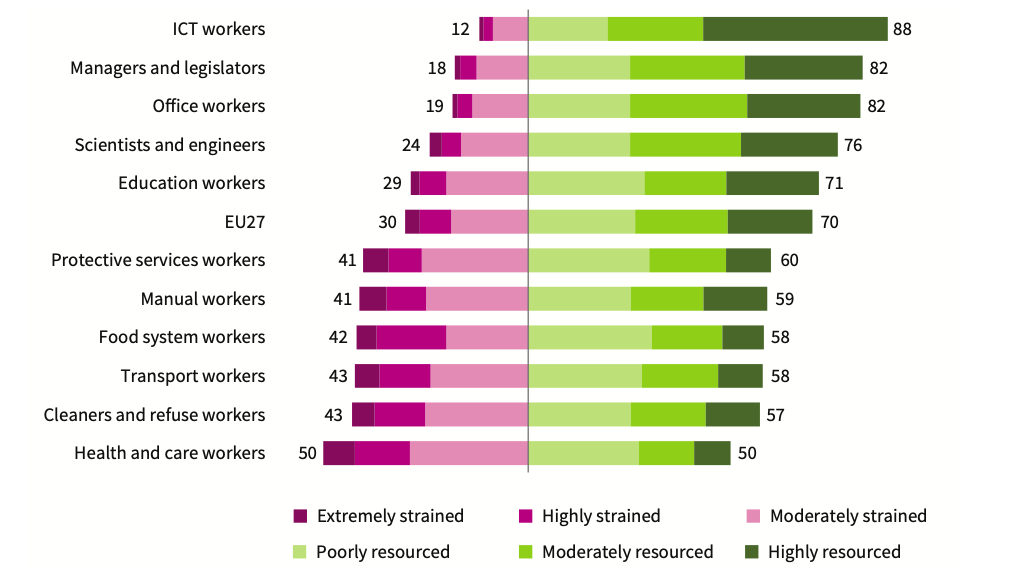
Source[8]
All major European surveys as well as several national studies highlight the prevalence and incidence of psychosocial risk factors in the health and social care sector. The European survey of enterprises on new and emerging risks (ESENER 2019) highlighted that psychosocial risk factors are reported more often in the health and social care sector than in other sectors (table 1)[10]. These results are in line with findings from workers’ surveys in Europe such as the European Working Conditions survey9 and the Labour Force Survey[3].
Table 1: Reported psychosocial risk factors (% of establishments) – ESENER 2019
| Human health and social activities | All |
| Pressure due to time constraints | 58% | 45% |
| Poor communication or cooperation within the organisation | 28% | 18% |
| Fear of job loss | 11% | 13% |
| Having to deal with difficult customers, patients, pupils etc. | 84% | 60% |
| Long or irregular working hours | 31% | 22% |
Source[10]
The EU-OSHA report, Human Health and Social Work Activities – Evidence from the European Survey of Enterprises on New and Emerging Risks[2], highlights that psychosocial risks are prevalent in the health and social care sector and have been exacerbated by the COVID-19 pandemic. Interviewees pointed to a significant increase in stress among healthcare workers, caused by factors such as overwork due to rising patient numbers and staff shortages, lack of personal protective equipment (PPE) during the first wave of COVID-19, and anxiety about their own health and the health of their families due to potential exposure to the virus at work.
Prevalence of harassment and violence
The health and social care sector also has the highest reported exposure to harassment and violence at work in the EU. Data from the EWCTS 2021[9] indicates that the health sector reported the highest percentage of workers subjected to all of the adverse social behaviour indicators:
- Verbal abuse (men: 17%, women: 18%)
- Bullying, harassment, violence (men: 11%, women: 11%)
- Unwanted sexual attention (men: 2,5%, women: 4,8%)
Results from the 2022 OSH Pulse survey[11] show that up to 30% of health and care sector respondents reported exposure to third-party violence and verbal abuse. This rate is significantly higher than the average for all sectors, which stands at 16%[11]. Research indicates that workers in emergency and psychiatric departments are particularly vulnerable to violence[12] [13] [14]. While most incidents involve verbal abuse, a substantial number also include physical assault, battery, stalking, or sexual harassment[15]. Studies also show that nurses are more susceptible to third-party violence and verbal abuse than physicians and other healthcare professionals, likely due to their greater accessibility to patients and their families[13] .
A study[16] carried out in 2016 in 5 European countries (Poland, the Czech Republic, the Slovak Republic, Turkey, and Spain) assessed physical and non-physical acts of workplace violence towards nurses working in the health sector. 54% of the respondents stated that they had been exposed to non-physical violence and 20% had been exposed to physical violent acts. The most common perpetrators were patients and patients’ relatives. In about 70% of these cases, no actions were taken after the act of violence to investigate its causes. 1 out of 2 respondents indicated that they did not report workplace violence as they believed it was useless or not important. This shows that workplace violence is often seen by nurses as an occupational hazard and, as such, it remains not reported. Acknowledgement of workplace violence is the first and important step towards prevention[16].
The OSH Pulse survey highlights that health and social care workers are not only the most exposed to third-party violence but also face the highest rates of harassment and bullying from co-workers, with 10% of healthcare workers affected compared to 7% across all sectors[11] [6]. In addition to individual risk factors like gender, education level, and work experience, organisational factors such as high workloads, rigid hierarchical structures, high stress levels, understaffing, and unhealthy competition among professionals play an important role[17].
Impact of psychosocial hazards on mental and physical health of healthcare workers
Work-related psychosocial risks can lead to significant stress and result in a range of serious mental and physical health issues, including chronic fatigue, sleep disorders, anxiety, musculoskeletal problems, migraines, burnout, depression, and cardiovascular diseases[6][7]. According to the EU-OSHA’s OSH Pulse survey (2022), 30% of health and social care sector respondents reported experiencing work-related stress, depression, or anxiety in the past 12 months. Additionally, 41% of healthcare workers reported overall fatigue, compared to 37% across all sectors[6]. Similar trends are evident in the EWCTS 2021 survey, which shows that healthcare workers, more than any other essential worker groups, suffer from a combination of physical and emotional exhaustion that often leads to burnout (figure 2)[8]. Studies have indicated that there is a high prevalence of burnout among both nurses and physicians[6].
Figure 2: Risk of burnout, by worker group, EU - EWCTS 2021 (%)
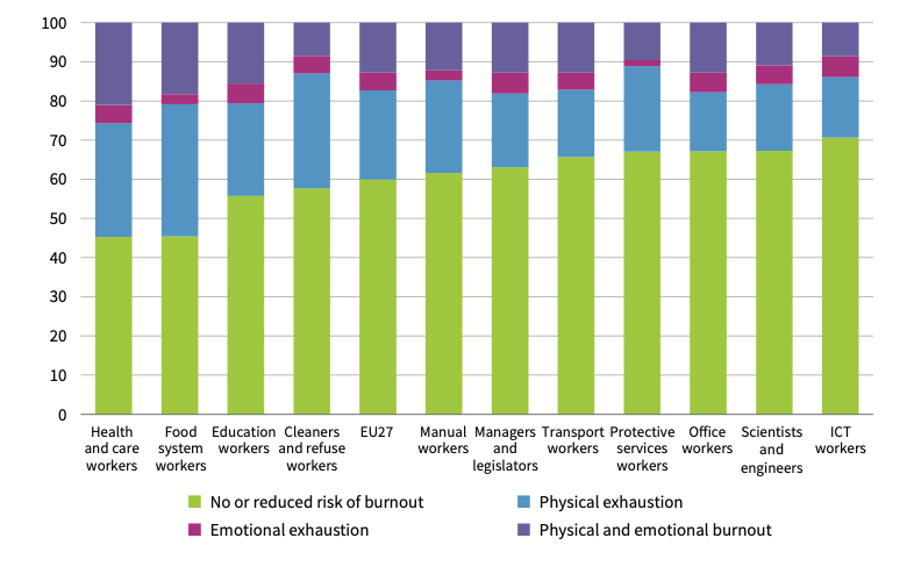
Source[8]
Research further indicates that increased workloads among healthcare workers are directly linked to poorer health outcomes[18]. For instance, a systematic review and meta-analysis of studies on hospital nurses found that each additional patient per registered nurse was associated with a 7% increase in burnout risk and a 5% increase in the likelihood of leaving the profession[19]. Another systematic review of intensive care nurses revealed that when nurse staffing levels are low—meaning a higher patient-to-nurse ratio—levels of burnout, stress, and fatigue can increase dramatically, ranging from 127% to 178%[20].
Promoting mental health in the health care sector
The Luxembourg Declaration on Workplace Health Promotion (WHP)[21] states that WHP “can be achieved through a combination of improving work organisation and the working environment, promoting active participation, and encouraging personal development." EU-OSHA also emphasises that “there is no point in implementing a WHP programme without also offering a safe and healthy working environment. WHP is based on a healthy culture first of all requiring proper risk management"[22] Mental health promotion is ‘the process of enhancing protective factors that contribute to good mental health’[23]. The European Pact for Mental Health and Well-being recommends the implementation of mental health and well-being programmes based on risk assessment and defining preventive actions addressing work-related psychosocial risks factors as well as early intervention schemes[24]. These interventions need to focus on areas both on individual level (person-directed) and on organisational level (work-directed). It is important to build a organisational culture in which mental health issues are not taboo. There are several types of interventions that can be used to reduce psychosocial risk factors and promote mental health in the health care. They are outlined in the following sections.
Work-directed interventions
Interventions directed at factors at work, or work-directed interventions typically contain measures to change the working environment and work organisation (work tasks or working methods)[25]. Interventions at organisational level are aimed at changing the structure of the organisation and/or at changing physical and environmental factors. These interventions try to reduce negative elements in the work organisation. These interventions are meant to eliminate the causes of stress at work[26]. Stressors can be assessed through a psychosocial risk analysis. The analysis will show which elements in the organisation (at task, team or organisational level) are critical and need improvement. Examples of organisational level interventions in the healthcare sector include[26] [18]:
- improved staffing levels during peak hours; this enables a reduction in workloads, improvements in organising shifts, and absence and contingency cover;
- specifying functions and responsibilities; for example, in nursing auxiliaries, for dispensing assistance with medication, and assistance and backup for providing treatment;
- supportive work environment, i.e. support of work colleagues to prevent mental health problems and the promotion of wellbeing
- external support networks
- improving autonomy and decision-making;
- promoting worker participation through meetings, enabling them to contribute suggestions, ideas and opinions;
- fair rewards.
Many organisations are already actively taking steps to prevent psychosocial risks in the healthcare sector. Data from ESENER[2] show that 3 out of 4 organisations in the healthcare sector have taken measures to improve job control and allow health and care workers to make decisions about how they do their work. Measures to address the problem of long and irregular working hours are less common (see figure 3).
Figure 3: Measures taken to prevent psychosocial risks (% of establishments in the health and social care sector – NACE Q. Base: all establishments in the Q sector in the EU-27 with 20 or more employees)
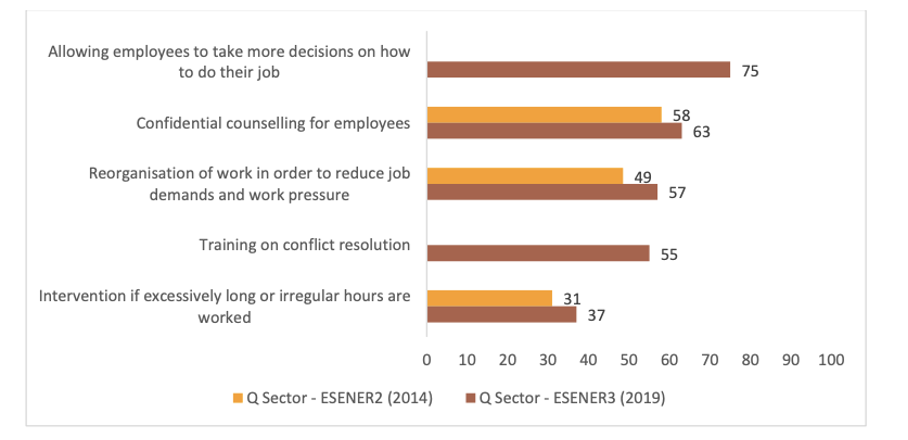
Source[2]
Person-directed interventions
Interventions focusing on people, or person-directed interventions, aim at teaching personal skills, techniques or remedies to decrease the effects of stressors at the individual level. For example, interventions aimed at mitigating the effects of stress by relaxation techniques or cognitive-behavioural techniques that increased coping skills, without changing the work environment or work tasks[25]. These interventions try to increase the workers’ resources and their ability to tackle stress. The employer should invest in interventions to increase the coping capacity of his employees, for example via training. However, it’s important to mention that interventions at organisational level should always come first and only when there is no solution or no way to totally eliminate certain risks, individual level interventions should be considered. Examples of such interventions include[23] [26]:
- improving relationships between colleagues and managers at work;
- establishing support groups;
- improving person-environment fit;
- clarifying role issues;
- increasing participation and autonomy;
- training to enhance employees’ self-esteem and self-worth, sense of belonging;
- learning coping strategies;
- cognitive-behavioural training;
- a Mindfulness-based stress reduction programme: this programme consists of a training to improve communication skills, learn how to deal with stress reactions, self-compassion;
- training to improve practical skills to reduce stress, to improve relation and functioning with patients, and coping with violent behaviours;
- staff training in coping with situations experienced such as death, pain and the terminally ill.
Effectiveness of interventions
Although interventions to address psychosocial risks in health and social care workers have been developed and studied, evidence of effectiveness remains scarce. Some of the key methodological deficiencies and limitations observed in the literature relate to research design, outcome measures, follow-up period and process evaluation and it is not always possible to determine clearly which outcomes are the actual results of an intervention[27] [28] [29]. Taking these limitations into consideration systematic meta-analyses and qualitative analyses of studies on mental health promotion interventions in the healthcare sector conclude that that organisational interventions reduce the levels of stress, burnout, and general ill health symptoms while person-directed interventions among health care workers effectively reduce the levels of burnout, anxiety, and stress[25] [30].
Several studies have shown that individual-focused interventions, such as educational interventions, mindfulness-based interventions, relaxing exercises have the potential to reduce occupational stress and/or burnout[31] [32] [33]. The results of one study[34] showed that psychosocial training (e.g., about attitudes and communication skills) reduced stress when compared with no intervention. Other studies[35] [36] [37] also indicate that person-directed interventions significantly reduced anxiety when compared with no intervention. It has also been found that a combination of training knowledge and skills and individual programme-planning decreased general symptoms of psychological distress[38].
Organisational interventions such as increased worker participation, and support provided by managers have also reported to be effective in reducing stress and improving general health. According to a study[39], support and advice given by nurse managers or quality-care coordinators reduced burnout symptoms. An evaluation of a caregiver support programme which was designed to increase participation and social support in work-related decision-making for caregiver teams in (mental) healthcare facilities indicated that the programme effectively increased the ability of teams of caregivers to mobilise socially supportive team behaviour and problem-solving techniques which strengthened participants’ belief and perception that they were able to cope with disagreements and overload at work, and enhanced the team climate, mental health and job satisfaction[40]. Studies have also shown[18] that creating a supportive work environment, for example by providing built-in, scheduled opportunities for a team to check in on each other's wellbeing, providing peer support during shifts, and organising weekly review meetings to address issues that impact on wellbeing, are effective interventions to address psychosocial risks and promote the mental wellbeing of healthcare workers.
While traditionally, stress prevention and management initiatives have exclusively focused on one type of intervention, the evidence indicates that to successfully prevent and manage work-related stress, intervention strategies should comprehensively incorporate elements work-directed and person-directed interventions. Specifically, they should address the root causes of work-related stress (primary prevention); provide training to managers and employees on stress management in order to reduce its impact (secondary prevention); and, for those that have suffered ill health as a result of work-related stress, provide them with resources to manage and reduce their respective effects (tertiary prevention)[41] [42].
Tackling violence and harassment in the healthcare sector
In 2002, the International Labour Office, International Council of Nurses, World Health Organization and Public Services International published through a joint programme on workplace violence in the health care sector the framework guidelines for addressing workplace violence in the health sector[43]. These guidelines provide comprehensive strategies for addressing various forms of workplace violence in the health sector, including physical and psychological violence. Although the ILO has not issued a new version, the guidelines remain an important resource for developing policies and interventions to protect healthcare workers. In particular, the guidelines emphasise the creation of a human-centred workplace culture, the involvement of all stakeholders in preventive measures, and the prioritisation of dignity and non-discrimination. In this respect, the guidelines are in line with the ILO Convention on Violence and Harassment (No. 190)[44], published in 2019, and related supporting guidance on the broader topic of violence and harassment in the world of work.
On an organisational level the following interventions can be taken[45] [43] [46] [15]:
- information and education on harassment (bullying, mobbing) and its consequences;
- guidelines — containing information on the nature and extent of the problem and its effects on health and quality of life;
- code of ethics — charter with indications that the company will not tolerate violence, harassment, unethical acts and discrimination;
- measures focused on patients and patients’ relatives e.g. information on the organisation of care, procedures, etc., reduction of waiting times, offering comfortable physical conditions such as private rooms,
- employment contracts — terms should be included in the contracts, regulating the matter and applying sanctions for any breach of the rules.
- developing a human-centred workplace culture and issuing a policy statement in which is clearly stated that violence or aggression against health care staff is not tolerated; all parties involved should be aware of the policy: patients, employees and managers;
- commitment to prevent violence and harassment;
- clear information and communication;
- conduct risk assessments on violence, aggression and harassment at work;
- control of the work environment: securing safety by using effective technology and procedures (e.g. alarm systems, security cameras, create distance between client/patient and staff by using a deeper counter, improved lighting, etc.);
- information on necessary precautions, on increased risks with certain patients, etc.
- establishing procedures for reporting and recording of all incidents of violence and aggression.
On an individual level the following steps can be taken[45] [43] [46] [47]:
- pre-incident training of staff on how to recognise actual or possible threats in the workplace; training of staff on how to react in violent situations.
- assistance and support (through designated confidantes, colleagues or managers)
- conflict resolution and mediation assistance
- to recognise the aggression, and, if necessary, to modify their own behaviour
- counselling;
- grievance procedures;
- debriefing (e.g. by establishing consciousness-raising groups that bring together people who have suffered from violence or harassment in different situations. Sharing similar experiences in a group allows the targets to realise that they are not the ones responsible for the event)
- rehabilitation for staff who were victim of a violence incident.
Conclusion
Evidence from the workplace case studies strongly suggests that implementing a mental health programme in the workplace has a great potential to generate economic returns and improve the mental health of the workforce[48]. However, due to the range of programmes and the different methodologies applied, no consistent evidence was found in the literature to support any one particular type of programme or approach. It’s important to find the best fitting approach according to the establishment’s characteristics. Smaller entities, like e.g. a doctor’s surgery need a different approach from large companies like e.g. hospitals.
Comprehensive mental health promotion interventions exist, though often organisations do not pay equal attention to all intervention levels[27]. In order to implement a good mental health promotion policy, any organisation needs to approach this topic from a holistic point of view by implementing actions on all levels with both employers and employees working together[49]. As the causes of mental ill health are multifactorial (e.g. a combination of staffing issues, workloads, work organisation issues and physical working conditions) all of these causes need to be tackled together for an intervention to be effective[49].

