Introduction
The models used in accident investigation can typically be grouped into three types: sequential, epidemiological, and systemic models. Although the sequential and epidemiological models have contributed to the understanding of accidents, they are not suitable for clarifying the complexities and dynamics of modern sociotechnical systems. In these systems, the interactions and events are connected in complicated ways, and standard safety engineering techniques alone are not sufficient to comprehend the accident causation. When analysing major accidents in process industries, a more systematic and professional model is needed than when supervisors and workers are investigating a normal minor accident in a simple setting.
The purpose of accident investigation
There are several definitions for accidents. In the context of accident investigation, here we will use the definition that an accident is an unplanned, unwanted, but controllable event which disrupts the work process and inflicts injuries.
An accident investigation may have different purposes[1]:
- Identify and describe the true course of events (what, where, when)
- Identify the direct and root causes / contributing factors of the accident (why)
- Identify risk reducing measures to prevent future, comparable accidents (learning)
- Investigate and evaluate the basis for potential criminal prosecution (blame)
- Evaluate the question of guilt in order to assess the liability for compensation (pay)
In an accident investigation, one tries to obtain answers to the following questions: what happened, why it happened, and how could this have been prevented?
An accident investigation should adopt a systematic approach to identify the factors leading to the accident, and in addition, it should examine what improvements are needed in the work environment and in organisational procedures as well as clarifying the responsibilities of each participant. The use of a systematic approach provides reliability to the investigation and allows a comprehensive description of the accident process and all factors influencing the accident. In brief, one needs to have rules of conduct for an investigation: who should participate and how to implement the investigation in practice.
After every incident and accident, decisions must be made about what kind of safety measures, guidance, training and information are needed in the workplace to prevent the similar incidents and who should deal with this information in the first place.
Main techniques for accident investigations and analyses
Simple techniques
Simple accident investigation techniques do not require the users to be a safety professional, i.e. learning these techniques do not require a long period of training or a certified degree. Learning to apply simple techniques only requires orientation and commitment. A typical feature for a simple technique is that the time required is not excessive, it should only take a couple of hours to perform this kind of accident investigation. A good example of these simple techniques is the Finnish model for accident investigation[2]. The Finnish model for accident investigation is not statutory, but it is a practical and easy to use tool for accident investigation at workplaces that can be used by non-experts.
In the Finnish model for accident investigation, it is recommended that the accident investigation should be conducted in working groups that include individuals from different levels of the organisation. Answers should be sought to such questions as:
- What happened (description)?
- Where did it happen?
- What were the circumstances at the accident scene?
- Which persons, machines, equipment were involved in the accident?
- What work was being performed when the accident occurred?
- Was there anything unusual in the situation?
The Finnish model for investigating occupational accidents consists of 10 steps:
- Orientating to the accident case: After an accident has occurred, it is essential to check the scene immediately in order to gather information about what happened. Eyewitnesses should be interviewed and circumstances can be photographed. All unusual and deviant events and occurrences should be recognised and reported. For example, checking the scene of the accident should include the following points:
- The names and locations of victim(s), eyewitnesses, and other persons who were working in the area;
- What was being done and which equipment was being used;
- The circumstances at the accident scene;
- The circumstances of the wider working environment in general (i.e. lighting, noise, and etc.);
- The level of training of the personnel involved;
- Organisation of the work and responsibilities of the persons involved.
- Describing the events in chronological order: The events should be outlined and separated. An easy way to undertake this description is to start with the accident itself. It is not enough just to describe the event that led to the accident. The investigation must identify all preceding work actions and go back to the very first one:
- What were the previous events before the accident occurred?
- What was the result? (injury type and injured body part)
- What was the type of the accident?
- What was the concrete cause of the injury?
- Gathering information on how the victim was involved, with the cause of the injury:
- The scene and occasion;
- What was he/she doing before the accident happened.
- Gathering information on how the cause of the injury was related to the accident cause: The cause of the injury may exist as a part of normal operations, but alternatively it may as well be caused because of broken or malfunctioning machines and/or equipment, or equipment wrongly placed in the workplace.
- Gathering information on contributing factors, i.e. what were the factors that contributed to the accident:
- Contributing factors, such as described in step 2, should be considered for each event;
- Each event may include more than one contributing factor;
- Recognition of contributing factors is based on careful inspection at the actual accident scheme, instead of guessing behind the office desk.
- Gathering information on why did the cause of the injury exist and how did it come to be present at the accident scene, especially when it is not its permanent location. One should also consider what were the accident factors contributing to the existence of the cause of the injury.
- Considering ways on how to prevent similar accidents occurring again.
- Choosing the best measures for preventing similar accidents in the future and considering how best to implement these measures:
- When several optional measures exist, it is essential to consider which one is the best and most realistic for being implemented.
- Choose the person responsible for implementing these measures;
- Set a schedule for the implementation.
- Distributing information on the results of the accident investigation at the workplace: It is essential to inform also other departments in addition to those where the accident took place, because similar accidents may occur in other locations as well.
- Follow-up: monitor the implementation of the measures and evaluate their impact.
Advanced techniques
Examples of more complex and systematic accident investigation techniques are AcciMap, STAMP model, MTO-analyses and FRAM method. Each of these advanced techniques requires specialised training.
The AcciMap
The AcciMap accident analysis technique is based on Rasmussen’s risk management framework[3] [4]. According to this framework, accidents in sociotechnical systems result from a control problem. Rasmussen's structure of risk management in sociotechnical systems consists of several levels, from the legislator to the operator (top-down) of the system[5]. Initially, different accident scenarios are selected, and the causal chains of events are analysed using a cause-consequence chart. A cause-consequence chart represents a generalisation that aggregates a set of accidental courses of events. Cause consequence charts have been widely used as the basis for predictive risk analysis[6]. See figure 1.
Figure 1. AcciMap method
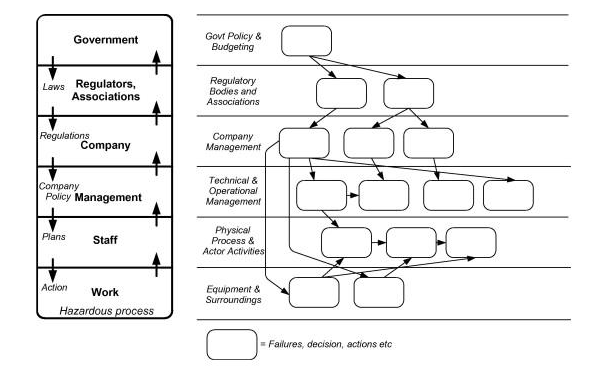
The set that is chosen to be included in a cause-consequence chart is defined by the choice of the critical event, which reflects the release of a well-defined hazard source, such as “loss of containment of hazardous substance", or “loss of control of accumulated energy". The critical event connects the causal tree (the logic relation among potential causes) with the subsequent event tree. In this way, the AcciMap serves to identify relevant decision-makers and the normal work situation in which they influence and modulate possible accidents.
The focus of AcciMap is not on the traditional search for identifying the “guilty person", but on the identification of those people in the system that can make decisions resulting in improved risk management, and hence, to the design of improved system safety[7] [8].
STAMP
STAMP (Systems Theoretic Accident Modeling and Processes) focuses on the role of constraints in safety management. Instead of defining safety in terms of preventing component failure events, safety is defined as a continuous control task to impose the constraints necessary to limit system behaviour to ensure only safe changes and adaptations. Accidents are seen as resulting from inadequate control or enforcement of constraints on safety-related behaviour at each level of the system development and system operations control structures. Therefore, accidents can be understood in terms of why the controls that were in place did not prevent or detect maladaptive changes (e.g. identifying the safety constraints that were violated at each level of the control structure, as well as why the constraints were inadequate or, if they were potentially adequate, why the system was unable to exert appropriate control over their enforcement).
The process leading to an accident (loss event) can be described as an adaptive feedback function that fails to maintain safety as performance changes over time to meet a complex set of goals and values. This adaptive feedback mechanism allows the model to incorporate adaptation as a fundamental property[9].
MTO-analysis
The basis for the MTO-analysis (Man, Technology and Organization) is that human, organisational, and technical factors are equally important in an accident investigation. The method is based on Human Performance Enhancement System (HPES)[1]
The MTO-analysis is based on three methods:
- Structured analysis by use of an event- and cause-diagram;
- Change analysis by describing how events have deviated from earlier events or common practice;
- Barrier analysis by identifying technological and administrative barriers, which have failed or are missing.
The first step in an MTO-analysis is to develop the event sequence in a longitudinal sequence and to illustrate the event sequence in a block diagram. The next step is to identify possible technical and human causes of each event and to draw these vertically into each event in the diagram. The third step is to analyse which technical, human or organisational barriers that have failed or were missing during the accident and illustrate all missing or failed barriers below the events as shown in the figure (Figure 2).
Figure 2. MTO diagram
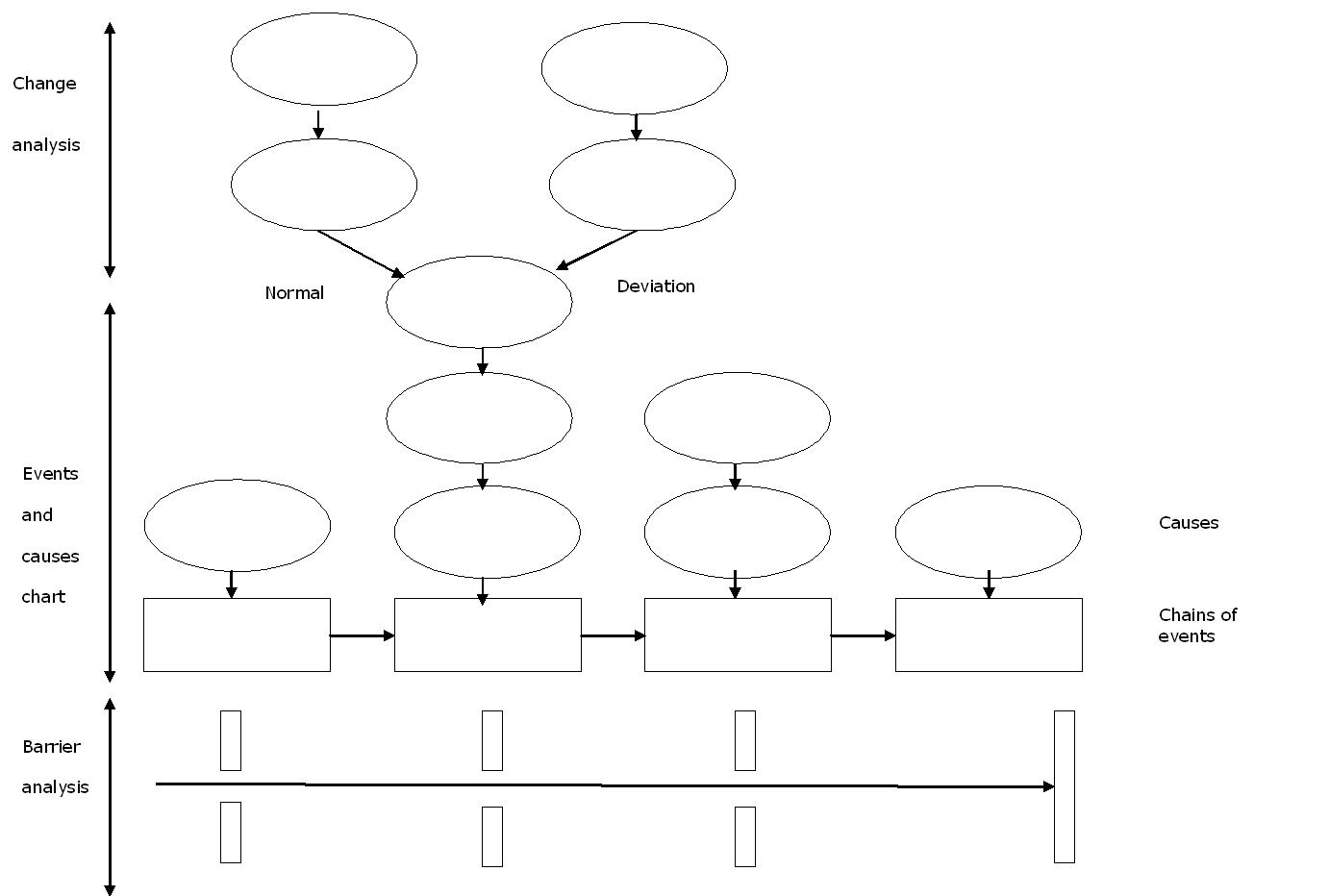
A checklist for identification of failure causes is also part of the MTO-methodology. The checklist contains the following factors: work organisation, work practice, management of work, change procedures, ergonomic/ deficiencies in the technology, communication, instructions/procedures, education/competence, and work environment. For each of these failure causes, there is a detailed checklist for basic or fundamental causes.
FRAM
FRAM and the associated method provide a way to describe how multiple functions and conditions can combine to produce an adverse outcome1. FRAM, originally an acronym for Functional Resonance Accident Model, has evolved into the Functional Resonance Analysis Method, reflecting its broader applicability beyond accident analysis to encompass complex socio-technical systems in general[10].
FRAM can be applied in two main ways:
- Retrospective analysis, i.e. analyses of accidents or other events;
- Prospective analysis, i.e. mainly analyses of current work domains or envisioned scenarios for risk management, or other types of performance management[10].
In retrospective analyses, FRAM is used to uncover potential systemic failures or critical underlying factors within specific work environments. These investigations typically begin with reports or audits of incidents to understand how adverse outcomes developed, and how different system components either mitigated or amplified the effects within the socio-technical system. Initially introduced to evaluate accidents in complex systems, FRAM focuses on how different system functions interact and may collectively contribute to accidents. In this context, "functions" refer to tasks, activities, or components that the system uses to achieve its goals. FRAM facilitates the analysis of the complex, non-linear relationships between functional activities by focusing on operational perspectives and the inherent variability and unpredictability of system functions. The approach allows for a comprehensive evaluation of how functions interact dynamically, offering insights into how they can lead to potential failures.
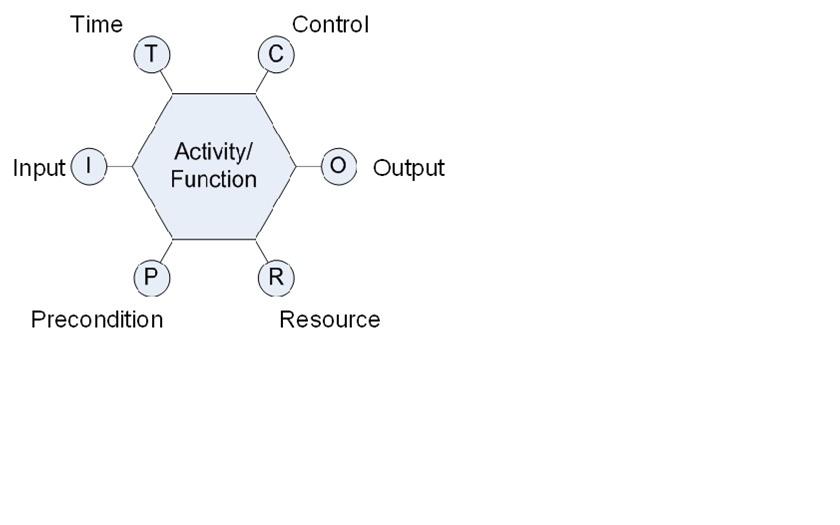
The figure below presents a schematic of a FRAM module, where each system function is represented by a hexagonal shape with six aspects: I for input, O for output, P for precondition, R for resource, T for time, and C for control[5] [10]. FRAM-based software[11] is available to support analysing system performance using FRAM.
Figure 3. A FRAM module describing an activity or function in terms of six aspects
Selecting a suitable accident investigation technique
It is essential that workplaces have a plan about how to investigate accidents. Irrespective of the technique, it is important that those persons who are involved in accident investigation know how to conduct the investigation and are aware of the guidelines for investigating accidents in their workplace. The persons who participate in these investigations should be named (usually safety managers and supervisors) and in addition, a worker from the accident scene may beneficially be included in the investigation.
When selecting a suitable technique for accident investigation, there should be at least one person who has a good knowledge about the different accident investigation techniques suitable for use in their work environment, and who is able to choose the proper method for each case. Some minor accidents may not need to be investigated in the same kind of depth as those that have led to serious injuries.
Conclusions
Accidents and also near misses almost never result from one single cause, most accidents involve multiple, interrelated causal factors. All actors or decision-makers influencing the normal work process might also influence accident scenarios, either directly or indirectly. This complexity should also be reflected in the accident investigation process. The aim of accident investigations should be to identify the sequence of events and all (causal) factors influencing the accident scenario in order to propose risk reduction measures that may prevent future accidents[1].
Often, accident investigations involve using a set of accident investigation methods. Each method might have different purposes and may make their own contribution to the total investigation process. It is important to remember that every piece of a puzzle is as significant as the others.
Graphical illustrations of the event sequence are useful during the investigation process because they provide an effective visual aid that summarises key information and provides a structured method for collecting, organising and integrating collected evidence to facilitate communication between the investigators. Graphical illustrations also help to identify information gaps[1].
During the investigation process, different methods should be used in order to analyse emerging problem areas. There should be at least one member of the multi-disciplinary investigation team who has good knowledge about the different accident investigation methods, and is able to choose the optimal methods for analysing the different problems[1].

