

The healthcare sector is large, employing around 11% of workers in the European Union[1]. Employment in the healthcare sector (Nace Q86) increased by 20% between 2008 and 2023 compared to only 5% increase in total employment[1]. Hospitals are the primary employer of healthcare workers, while other employers include medical practices, nursing and care homes and other healthcare activities such as homecare services[2]. The evidence indicates that mental health issues are of increasing concern in the healthcare sector and a number of initiatives have been implemented to address these issues. This article provides an overview of the factors which pose a threat to the mental health of workers in the sector and identifies and evaluates interventions used for promoting the mental health of healthcare workers.
While exposure to factors affecting mental health substantially varies across all economic sectors, exposure occurred most often in the sector ‘human health and social work activities’ with 58,5% of the workers in the sector reporting to risk factors affecting their mental health[3]. Mental health is described by the World Health Organization[4] as ‘a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’. In this positive sense, mental health is the foundation for well-being and effective functioning for an individual and for a community. Mental health and mental illnesses are determined by multiple and interacting social and psychological factors, including psychosocial hazards, which are prevalent in all workplaces. Psychosocial risks refer to the likelihood that work-related psychosocial hazards will have a negative impact on employees’ health and safety through their perceptions and experience[5].
Many work-related psychosocial hazards exist. Those which are typical for the health care sector[6] [7] include amongst others:
Data from the European Working Conditions Telephone Survey (EWCTS 2021) indicate that half of health and social care workers are in "strained jobs" according to the Job Quality Index[8]. This index assesses job quality by comparing the number of demands and resources associated with a job, incorporating indicators from six key dimensions: physical and social environment, job tasks, organisational characteristics, working time arrangements, job prospects and intrinsic job features. Job quality is determined by the difference between the number of job resources and job demands. A job is considered as "strained" when demands exceed resources, while it is considered "resourced" when resources outweigh demands[9].
Figure 1: Job quality index, by worker group, EU - EWCTS 2021 (%)
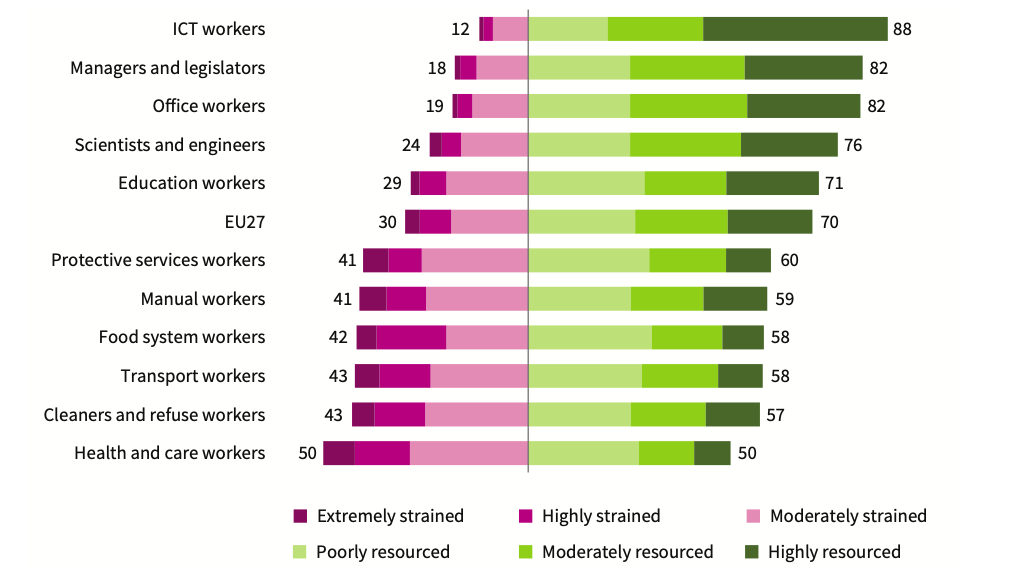
Source[8]
All major European surveys as well as several national studies highlight the prevalence and incidence of psychosocial risk factors in the health and social care sector. The European survey of enterprises on new and emerging risks (ESENER 2019) highlighted that psychosocial risk factors are reported more often in the health and social care sector than in other sectors (table 1)[10]. These results are in line with findings from workers’ surveys in Europe such as the European Working Conditions survey9 and the Labour Force Survey[3].
Table 1: Reported psychosocial risk factors (% of establishments) – ESENER 2019
| Human health and social activities | All | |
| Pressure due to time constraints | 58% | 45% |
| Poor communication or cooperation within the organisation | 28% | 18% |
| Fear of job loss | 11% | 13% |
| Having to deal with difficult customers, patients, pupils etc. | 84% | 60% |
| Long or irregular working hours | 31% | 22% |
Source[10]
The EU-OSHA report, Human Health and Social Work Activities – Evidence from the European Survey of Enterprises on New and Emerging Risks[2], highlights that psychosocial risks are prevalent in the health and social care sector and have been exacerbated by the COVID-19 pandemic. Interviewees pointed to a significant increase in stress among healthcare workers, caused by factors such as overwork due to rising patient numbers and staff shortages, lack of personal protective equipment (PPE) during the first wave of COVID-19, and anxiety about their own health and the health of their families due to potential exposure to the virus at work.
The health and social care sector also has the highest reported exposure to harassment and violence at work in the EU. Data from the EWCTS 2021[9] indicates that the health sector reported the highest percentage of workers subjected to all of the adverse social behaviour indicators:
Results from the 2022 OSH Pulse survey[11] show that up to 30% of health and care sector respondents reported exposure to third-party violence and verbal abuse. This rate is significantly higher than the average for all sectors, which stands at 16%[11]. Research indicates that workers in emergency and psychiatric departments are particularly vulnerable to violence[12] [13] [14]. While most incidents involve verbal abuse, a substantial number also include physical assault, battery, stalking, or sexual harassment[15]. Studies also show that nurses are more susceptible to third-party violence and verbal abuse than physicians and other healthcare professionals, likely due to their greater accessibility to patients and their families[13] .
A study[16] carried out in 2016 in 5 European countries (Poland, the Czech Republic, the Slovak Republic, Turkey, and Spain) assessed physical and non-physical acts of workplace violence towards nurses working in the health sector. 54% of the respondents stated that they had been exposed to non-physical violence and 20% had been exposed to physical violent acts. The most common perpetrators were patients and patients’ relatives. In about 70% of these cases, no actions were taken after the act of violence to investigate its causes. 1 out of 2 respondents indicated that they did not report workplace violence as they believed it was useless or not important. This shows that workplace violence is often seen by nurses as an occupational hazard and, as such, it remains not reported. Acknowledgement of workplace violence is the first and important step towards prevention[16].
The OSH Pulse survey highlights that health and social care workers are not only the most exposed to third-party violence but also face the highest rates of harassment and bullying from co-workers, with 10% of healthcare workers affected compared to 7% across all sectors[11] [6]. In addition to individual risk factors like gender, education level, and work experience, organisational factors such as high workloads, rigid hierarchical structures, high stress levels, understaffing, and unhealthy competition among professionals play an important role[17].
Work-related psychosocial risks can lead to significant stress and result in a range of serious mental and physical health issues, including chronic fatigue, sleep disorders, anxiety, musculoskeletal problems, migraines, burnout, depression, and cardiovascular diseases[6][7]. According to the EU-OSHA’s OSH Pulse survey (2022), 30% of health and social care sector respondents reported experiencing work-related stress, depression, or anxiety in the past 12 months. Additionally, 41% of healthcare workers reported overall fatigue, compared to 37% across all sectors[6]. Similar trends are evident in the EWCTS 2021 survey, which shows that healthcare workers, more than any other essential worker groups, suffer from a combination of physical and emotional exhaustion that often leads to burnout (figure 2)[8]. Studies have indicated that there is a high prevalence of burnout among both nurses and physicians[6].
Figure 2: Risk of burnout, by worker group, EU - EWCTS 2021 (%)
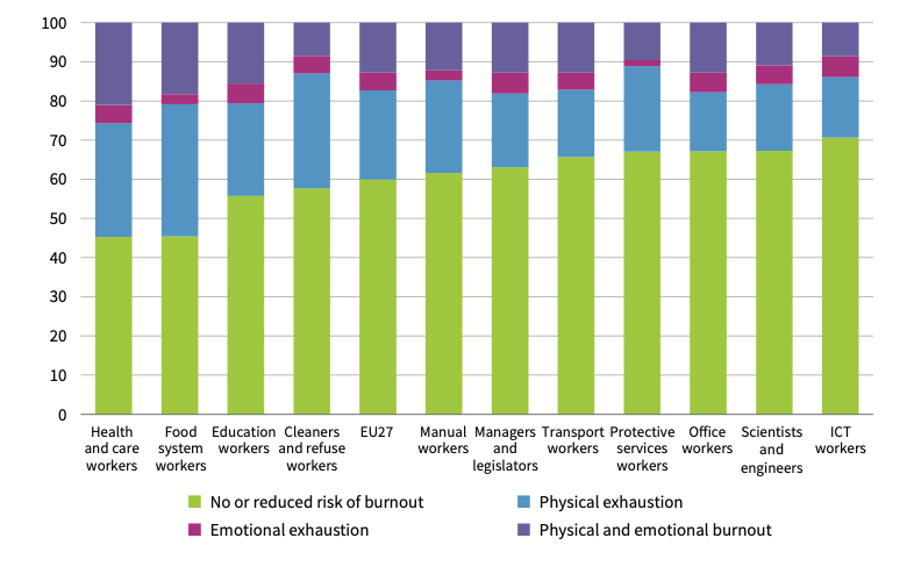
Source[8]
Research further indicates that increased workloads among healthcare workers are directly linked to poorer health outcomes[18]. For instance, a systematic review and meta-analysis of studies on hospital nurses found that each additional patient per registered nurse was associated with a 7% increase in burnout risk and a 5% increase in the likelihood of leaving the profession[19]. Another systematic review of intensive care nurses revealed that when nurse staffing levels are low—meaning a higher patient-to-nurse ratio—levels of burnout, stress, and fatigue can increase dramatically, ranging from 127% to 178%[20].
The Luxembourg Declaration on Workplace Health Promotion (WHP)[21] states that WHP “can be achieved through a combination of improving work organisation and the working environment, promoting active participation, and encouraging personal development." EU-OSHA also emphasises that “there is no point in implementing a WHP programme without also offering a safe and healthy working environment. WHP is based on a healthy culture first of all requiring proper risk management"[22] Mental health promotion is ‘the process of enhancing protective factors that contribute to good mental health’[23]. The European Pact for Mental Health and Well-being recommends the implementation of mental health and well-being programmes based on risk assessment and defining preventive actions addressing work-related psychosocial risks factors as well as early intervention schemes[24]. These interventions need to focus on areas both on individual level (person-directed) and on organisational level (work-directed). It is important to build a organisational culture in which mental health issues are not taboo. There are several types of interventions that can be used to reduce psychosocial risk factors and promote mental health in the health care. They are outlined in the following sections.
Interventions directed at factors at work, or work-directed interventions typically contain measures to change the working environment and work organisation (work tasks or working methods)[25]. Interventions at organisational level are aimed at changing the structure of the organisation and/or at changing physical and environmental factors. These interventions try to reduce negative elements in the work organisation. These interventions are meant to eliminate the causes of stress at work[26]. Stressors can be assessed through a psychosocial risk analysis. The analysis will show which elements in the organisation (at task, team or organisational level) are critical and need improvement. Examples of organisational level interventions in the healthcare sector include[26] [18]:
Many organisations are already actively taking steps to prevent psychosocial risks in the healthcare sector. Data from ESENER[2] show that 3 out of 4 organisations in the healthcare sector have taken measures to improve job control and allow health and care workers to make decisions about how they do their work. Measures to address the problem of long and irregular working hours are less common (see figure 3).
Figure 3: Measures taken to prevent psychosocial risks (% of establishments in the health and social care sector – NACE Q. Base: all establishments in the Q sector in the EU-27 with 20 or more employees)
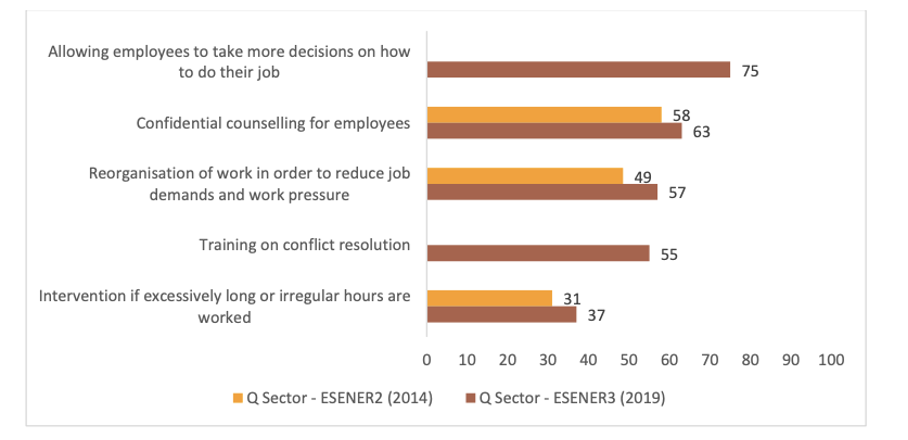
Source[2]
Interventions focusing on people, or person-directed interventions, aim at teaching personal skills, techniques or remedies to decrease the effects of stressors at the individual level. For example, interventions aimed at mitigating the effects of stress by relaxation techniques or cognitive-behavioural techniques that increased coping skills, without changing the work environment or work tasks[25]. These interventions try to increase the workers’ resources and their ability to tackle stress. The employer should invest in interventions to increase the coping capacity of his employees, for example via training. However, it’s important to mention that interventions at organisational level should always come first and only when there is no solution or no way to totally eliminate certain risks, individual level interventions should be considered. Examples of such interventions include[23] [26]:
Although interventions to address psychosocial risks in health and social care workers have been developed and studied, evidence of effectiveness remains scarce. Some of the key methodological deficiencies and limitations observed in the literature relate to research design, outcome measures, follow-up period and process evaluation and it is not always possible to determine clearly which outcomes are the actual results of an intervention[27] [28] [29]. Taking these limitations into consideration systematic meta-analyses and qualitative analyses of studies on mental health promotion interventions in the healthcare sector conclude that that organisational interventions reduce the levels of stress, burnout, and general ill health symptoms while person-directed interventions among health care workers effectively reduce the levels of burnout, anxiety, and stress[25] [30].
Several studies have shown that individual-focused interventions, such as educational interventions, mindfulness-based interventions, relaxing exercises have the potential to reduce occupational stress and/or burnout[31] [32] [33]. The results of one study[34] showed that psychosocial training (e.g., about attitudes and communication skills) reduced stress when compared with no intervention. Other studies[35] [36] [37] also indicate that person-directed interventions significantly reduced anxiety when compared with no intervention. It has also been found that a combination of training knowledge and skills and individual programme-planning decreased general symptoms of psychological distress[38].
Organisational interventions such as increased worker participation, and support provided by managers have also reported to be effective in reducing stress and improving general health. According to a study[39], support and advice given by nurse managers or quality-care coordinators reduced burnout symptoms. An evaluation of a caregiver support programme which was designed to increase participation and social support in work-related decision-making for caregiver teams in (mental) healthcare facilities indicated that the programme effectively increased the ability of teams of caregivers to mobilise socially supportive team behaviour and problem-solving techniques which strengthened participants’ belief and perception that they were able to cope with disagreements and overload at work, and enhanced the team climate, mental health and job satisfaction[40]. Studies have also shown[18] that creating a supportive work environment, for example by providing built-in, scheduled opportunities for a team to check in on each other's wellbeing, providing peer support during shifts, and organising weekly review meetings to address issues that impact on wellbeing, are effective interventions to address psychosocial risks and promote the mental wellbeing of healthcare workers.
While traditionally, stress prevention and management initiatives have exclusively focused on one type of intervention, the evidence indicates that to successfully prevent and manage work-related stress, intervention strategies should comprehensively incorporate elements work-directed and person-directed interventions. Specifically, they should address the root causes of work-related stress (primary prevention); provide training to managers and employees on stress management in order to reduce its impact (secondary prevention); and, for those that have suffered ill health as a result of work-related stress, provide them with resources to manage and reduce their respective effects (tertiary prevention)[41] [42].
In 2002, the International Labour Office, International Council of Nurses, World Health Organization and Public Services International published through a joint programme on workplace violence in the health care sector the framework guidelines for addressing workplace violence in the health sector[43]. These guidelines provide comprehensive strategies for addressing various forms of workplace violence in the health sector, including physical and psychological violence. Although the ILO has not issued a new version, the guidelines remain an important resource for developing policies and interventions to protect healthcare workers. In particular, the guidelines emphasise the creation of a human-centred workplace culture, the involvement of all stakeholders in preventive measures, and the prioritisation of dignity and non-discrimination. In this respect, the guidelines are in line with the ILO Convention on Violence and Harassment (No. 190)[44], published in 2019, and related supporting guidance on the broader topic of violence and harassment in the world of work.
On an organisational level the following interventions can be taken[45] [43] [46] [15]:
On an individual level the following steps can be taken[45] [43] [46] [47]:
Evidence from the workplace case studies strongly suggests that implementing a mental health programme in the workplace has a great potential to generate economic returns and improve the mental health of the workforce[48]. However, due to the range of programmes and the different methodologies applied, no consistent evidence was found in the literature to support any one particular type of programme or approach. It’s important to find the best fitting approach according to the establishment’s characteristics. Smaller entities, like e.g. a doctor’s surgery need a different approach from large companies like e.g. hospitals.
Comprehensive mental health promotion interventions exist, though often organisations do not pay equal attention to all intervention levels[27]. In order to implement a good mental health promotion policy, any organisation needs to approach this topic from a holistic point of view by implementing actions on all levels with both employers and employees working together[49]. As the causes of mental ill health are multifactorial (e.g. a combination of staffing issues, workloads, work organisation issues and physical working conditions) all of these causes need to be tackled together for an intervention to be effective[49].
[1] Eurostat, Database, Employment by sex, age and detailed economic activity (Labour Force Survey - lfsa_egan22d). Available at: https://ec.europa.eu/eurostat/web/main/data/database
[2] EU-OSHA – European Agency for Safety and Health at Work. Human health and social work activities – evidence from the European Survey of Enterprises on New and Emerging Risks (ESENER). Report, 2022. Available at: https://osha.europa.eu/en/publications/human-health-and-social-work-activities-evidence-european-survey-enterprises-new-and-emerging-risks-esener
[3] Eurostat. Self-reported work-related health problems and risk factors - key statistics. Statistics explained. Available at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Self-reported_work-related_health_problems_and_risk_factors_-_key_statistics
[4] WHO – World Health Organization. Mental health. Available at: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
[5] Cox, T., & Griffiths, A., ‘The nature and measurement of work-related stress: theory and practice’, In J.R. Wilson & N. Corlett (Eds.), Evaluation of Human Work (3rd ed.), CRS Press, London, 2005.
[6] EU-OSHA – European Agency for Safety and Health at Work. Psychosocial risks in the health and social care sector. Discussion paper, 2023. Available at: https://osha.europa.eu/en/publications/psychosocial-risks-health-and-social-care-sector
[7] Helfferich, B. Franklin, P. (2023). Work-related psychosocial risks in the healthcare and long-term care sectors. ETUI, The European Trade Union Institute. Available at: https://www.etui.org/publications/work-related-psychosocial-risks-healthcare-and-long-term-care-sectors
[8] Eurofound (2023), Job quality of COVID-19 pandemic essential workers, European Working Conditions Telephone Survey series, Publications Office of the European Union, Luxembourg. Available at: https://www.eurofound.europa.eu/en/publications/2023/job-quality-covid-19-pandemic-essential-workers
[9] Eurofound. Working conditions in the time of COVID-19: Implications for the future, European Working Conditions Telephone Survey 2021 series, 2022. Available at: https://www.eurofound.europa.eu/publications/report/2022/working-conditions-in-the-time-of-covid-19-implications-for-the-future
[10] EU-OSHA, ESENER 2019, Third European Survey of Enterprises on New and Emerging Risks. Available at: https://visualisation.osha.europa.eu/esener/en/survey/overview/2019
[11] EU-OSHA – European Agency for Safety and Health at Work. OSH Pulse - Occupational safety and health in post-pandemic workplaces. Report, 2022. Available at: https://osha.europa.eu/en/publications/osh-pulse-occupational-safety-and-health-post-pandemic-workplaces
[12] Chakraborty, S., Mashreky, S. R., & Dalal, K. (2022). Violence against physicians and nurses: a systematic literature review. Journal of Public Health, 30(8), 1837-1855.
[13] Yusoff, H. M., Ahmad, H., Ismail, H., Reffin, N., Chan, D., Kusnin, F., ... & Rahman, M. A. (2023). Contemporary evidence of workplace violence against the primary healthcare workforce worldwide: a systematic review. Human resources for health, 21(1), 82.
[14] Pagnucci, N., Ottonello, G., Capponi, D., Catania, G., Zanini, M., Aleo, G., ... & Bagnasco, A. (2022). Predictors of events of violence or aggression against nurses in the workplace: A scoping review. Journal of Nursing Management, 30(6), 1724-1749.
[15] Caruso, R., Toffanin, T., Folesani, F., Biancosino, B., Romagnolo, F., Riba, M. B., ... & Grassi, L. (2022). Violence against physicians in the workplace: trends, causes, consequences, and strategies for intervention. Current psychiatry reports, 24(12), 911-924.
[16] Babiarczyk B, Turbiarz A, Tomagová M, Zeleníková R, Önler E, Sancho Cantus D. Reporting of workplace violence towards nurses in 5 European countries – a cross-sectional study. International Journal of Occupational Medicine and Environmental Health. 2020;33(3):325-338. doi:10.13075/ijomeh.1896.01475.
[17] Pagnucci, N., Ottonello, G., Capponi, D., Catania, G., Zanini, M., Aleo, G., ... & Bagnasco, A. (2022). Predictors of events of violence or aggression against nurses in the workplace: A scoping review. Journal of Nursing Management, 30(6), 1724-1749.
[18] Narocki, C., Paula Franklin, P. (2022). Psychosocial risks in the healthcare and long-term care sectors. ETUI, The European Trade Union Institute. Available at: https://www.etui.org/publications/psychosocial-risks-healthcare-and-long-term-care-sectors
[19] Shin, S., Park, J. H., & Bae, S. H. (2018). Nurse staffing and nurse outcomes: A systematic review and meta-analysis. Nursing outlook, 66(3), 273-282, cited in [18]
[20] Bae, S. H. (2021). Intensive care nurse staffing and nurse outcomes: A systematic review. Nursing in Critical Care, 26(6), 457-466, cited in [18]
[21] Luxembourg declaration on workplace health promotion. Luxembourg:,. European Network for Workplace Health Promotion,1997 (updated in June 2005 and January 2007). Available at: https://www.enwhp.org/?i=portal.en.workplace-health-promotion
[22] EU-OSHA – European Agency for Safety and Health at Work. E-facts 93: Workplace Health Promotion for Employers. Factsheet, 2010. Available at: https://osha.europa.eu/en/publications/factsheet-93-workplace-health-promotion-employers
[23] Pollett, H., Mental health promotion: a literature review. Prepared for the Mental Health Promotion Working Group of the Provincial Wellness Advisory Council. June 18th 2007.
[24] European Pact for Mental Health and Wellbeing (2008). EU High Level Conference 'Together for mental health and wellbeing', Brussels, 12-13 June 2008. Available at: http://ec.europa.eu/health/ph_determinants/life_style/mental/docs/pact_en.pdf
[25] Ruotsalainen, J. H., Verbeek, J. H., Mariné, A., & Serra, C. (2014). Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews.
[26] EU-OSHA – European Agency for Safety and Health at Work. How to Tackle Psychosocial Issues and Reduce Work-Related Stress. Report, 2002. Available at: https://osha.europa.eu/en/publications/te4502967enc-how-tackle-psychosocial-issues-and-reduce-work-related-stress
[27] EU-OSHA – European Agency for Safety and Health at Work. Research on Work-related Stress. Report, 2000. Available at: https://osha.europa.eu/en/publications/report-research-work-related-stress
[28] Nikunlaakso, R., Selander, K., Oksanen, T., & Laitinen, J. (2022). Interventions to reduce the risk of mental health problems in health and social care workplaces: A scoping review. Journal of psychiatric research, 152, 57-69.
[29] de Wijn, A. N., & van der Doef, M. P. (2022). A meta-analysis on the effectiveness of stress management interventions for nurses: Capturing 14 years of research. International Journal of Stress Management, 29(2), 113.
[30] Aust, B., Møller, J. L., Nordentoft, M., Frydendall, K. B., Bengtsen, E., Jensen, A. B., ... & Jaspers, S. Ø. (2023). How effective are organizational-level interventions in improving the psychosocial work environment, health, and retention of workers? A systematic overview of systematic reviews. Scandinavian Journal of Work, Environment & Health, 49(5), 315.
[31] Tamminga, S. J., Emal, L. M., Boschman, J. S., Levasseur, A., Thota, A., Ruotsalainen, J. H., & Schelvis, R. M. (2023). Individual‐level interventions for reducing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews, (5).
[32] Estevez Cores, S., Sayed, A. A., Tracy, D. K., & Kempton, M. J. (2021). Individual-focused occupational health interventions: A meta-analysis of randomized controlled trials. Journal of Occupational Health Psychology, 26(3), 189.
[33] Xu, H. G., Kynoch, K., Tuckett, A., & Eley, R. (2020). Effectiveness of interventions to reduce emergency department staff occupational stress and/or burnout: a systematic review. JBI evidence synthesis, 18(6), 1156-1188.
[34] Delvaux, N., Razavi, D., Marchal, S., Bredart, A., Farvacques, C., & Slachmuylder, J.L., Effects of a 105 hours psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. British Jounal of Cancer, Vol 90, 2004, pp.106-114.
[35] Yung, P.M., Fung, M.Y., Chan, T.M., & Lau, B.W. Relaxation training methods for nurse managers in Hong Kong: a controlled study. International Journal of Mental Health Nursing, Vol 13, 2004, pp. 255-261.
[36] Jones, M.C., & Johnston, D.W. Evaluating the impact of a worksite stress management programme for distressed students: a randomised controlled trial. Psychology and Health, Vol 15, 15, pp. 689-706.
[37] von Baeyer C., & Krause L. Effectiveness of stress management training for nurses working in a burn treatment unit. International Journal of Psychiatry in Medicine, Vol 13,1983, pp.113-126.
[38] Proctor, R., Stratton-Powell, H., Tarrier, N., & Burns, A. The impact of training and support on stress among care staff in nursing and residential homes for the elderly. Journal of Mental Health, Vol 7, 1998, pp. 59-71.
[39] Melchior M.E., Philipsen, H., Abu-Saad, H.H., Halfens, R.J., van de Berg, A.A., & Gassman, P., The effectiveness of primary nursing on burnout among psychiatric nurses in long-stay settings;. Journal of Advanced Nursing, Vol 24, 1996, pp. 694-702.
[40] Jané-Llopis, E., Barry, M., Hosman, C. & Patel, V., Mental health promotion works: a review, Promotion & Education, Vol 2, 2005, pp. 9-25.
[41] Giga, S.I., Cooper, C.L. & Faragher, B., The development of a framework for a comprehensive approach to stress management interventions at work, International Journal of Stress Management, Vol 19, No 4, 2003, pp. 280-296.
[42] LaMontagne, A.D., Keegel, T., Louie, A.M.L., Ostry, A., & Landsbergis, P.A., A systematic review of the job-stress intervention evaluation literature, 1995-2005, International Journal of Occupational & Environmental Health, 13, 2007, pp. 268-280.
[43] International Labour Organization, International Council of Nurses, World Health Organization & Public Services International, Framework Guidelines for Addressing Workplace Violence in the Health Sector, International Labour Office, Geneva, 2002. Available at: https://apps.who.int/iris/handle/10665/42617
[44] ILO Convention N° 190 Violence and Harassment Convention, 2019. Available at: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C190
[45] EU-OSHA – European Agency for Safety and Health at Work. Workplace Violence and Harassment: a European Picture. Report, 2011. Available at: https://osha.europa.eu/en/publications/workplace-violence-and-harassment-european-picture
[46] WHO – World Health Organization, Raising awareness to psychological harassment at work. Protecting workers’ health series; no. 4, World Health Organization, Geneva, 2003. Available at: https://www.who.int/publications/i/item/9241590521
[47] Arnetz, J., & Arnetz, B. Implementation and evaluation of a practical intervention programme for dealing with violence towards health care workers, Journal of Advanced Nursing, Vol 31, No 3, 2000, pp. 668-680.
[48] EC – European Commission, Economic analysis of workplace mental health promotion and mental disorder prevention programmes and of their potential contribution to EU health, social and economic policy objectives, Final report Specific Request EAHC/2011/Health/19 for the Implementation of Framework Contract EAHC/2010/Health/01 Lot 2, EC Executive Agency for Health and Consumers. Available at: http://www.mentalhealthpromotion.net/resources/matrix_2012-economic-analysis-of-wmhp-programmes.pdf
[49] EU-OSHA – European Agency for Safety and Health at Work. Mental health promotion in the workplace –A good practice report. Report, 2011. Available at: https://osha.europa.eu/en/publications/mental-health-promotion-workplace-good-practice-report
EU-OSHA – European Agency for Safety and Health at Work. Human health and social work activities – evidence from the European Survey of Enterprises on New and Emerging Risks (ESENER). Report, 2022. Available at: https://osha.europa.eu/en/publications/human-health-and-social-work-activities-evidence-european-survey-enterprises-new-and-emerging-risks-esener
EU-OSHA – European Agency for Safety and Health at Work. Psychosocial risks in the health and social care sector. Discussion paper, 2023. Available at: https://osha.europa.eu/en/publications/psychosocial-risks-health-and-social-care-sector
EU-OSHA - European Agency for Safety and Health at Work. Healthy workers, thriving companies - a practical guide to wellbeing at work, 2018. Available at: https://osha.europa.eu/en/publications/healthy-workers-thriving-companies-practical-guide-wellbeing-work
EU-OSHA - European Agency for Safety and Health at Work. E-guide to managing stress and psychosocial risks. Available at: https://osha.europa.eu/en/tools-and-resources/e-guides/e-guide-managing-stress-and-psychosocial-risks
EU-OSHA - European Agency for Safety and Health at Work. Mental health promotion in the workplace – A good practice report, 2011. Available at: https://osha.europa.eu/en/publications/mental-health-promotion-workplace-good-practice-report/view
EU-OSHA - European Agency for Safety and Health at Work, E-fact 46: Mental health promotion in the health care sector, 2009. Available at: https://osha.europa.eu/en/publications/e-fact-46-mental-health-promotion-health-care-sector/view
European Commission: Directorate-General for Health and Food Safety, Opinion on supporting mental health of health workforce and other essential workers, Publications Office of the European Union, 2021. Available at: https://data.europa.eu/doi/10.2875/80970
Vybrat téma