

Work-related musculoskeletal disorders (MSDs) cover a broad range of health problems. These health problems range from discomfort, minor aches and pains to more serious medical conditions that can lead to permanent disability. Every year millions of European workers are affected by MSDs. The most well-known MSDs are low back pain and work-related upper limb disorders. The first is mainly associated with manual handling while the main risk factors for the latter are associated with task repetition and awkward work postures. Lower limb MSDs are also recognised as conditions that may be work-related. The causes of work-related MSDs are multifactorial and include physical, organisational and psychosocial risk factors[1].
Work-related MSDs are health problems that are mainly caused or aggravated by work and affect the muscles, tendons, ligaments, cartilage, the vascular system, nerves or other soft tissues and joints of the musculoskeletal system. They can affect the back, neck, shoulders and upper and lower limbs and range from minor aches and pains to more serious conditions requiring time off work or medical treatment. In more chronic cases, they can even lead to disability and the need to permanently stop working[2].
It is long recognised that work may adversely affect health. Almost three centuries ago (in 1717) the Italian physician Bernardino Ramazzini, father of occupational medicine acknowledged the relationship between work and certain disorders of the musculoskeletal system due to the performance of sudden and irregular movements and the adoption of awkward postures. Due to this fact some disorders assumed names related with the professions where they mainly occurred. Therefore, a variety of terms for MSDs can be found that directly refer to jobs and professions, for instance “carpenter’s elbow”, “seamstress’ wrist” or “bricklayer’s shoulder”[3].
Work-related MSDs associated with repetitive and strenuous working conditions continue to represent one of the biggest occupational problems in companies. Despite a variety of efforts to control them, including changes in workplace design, adjustments to work organisation and methods, and training programmes, work-related musculoskeletal disorders (MSDs) are a major source of human suffering and cost to businesses and to healthcare systems[4].
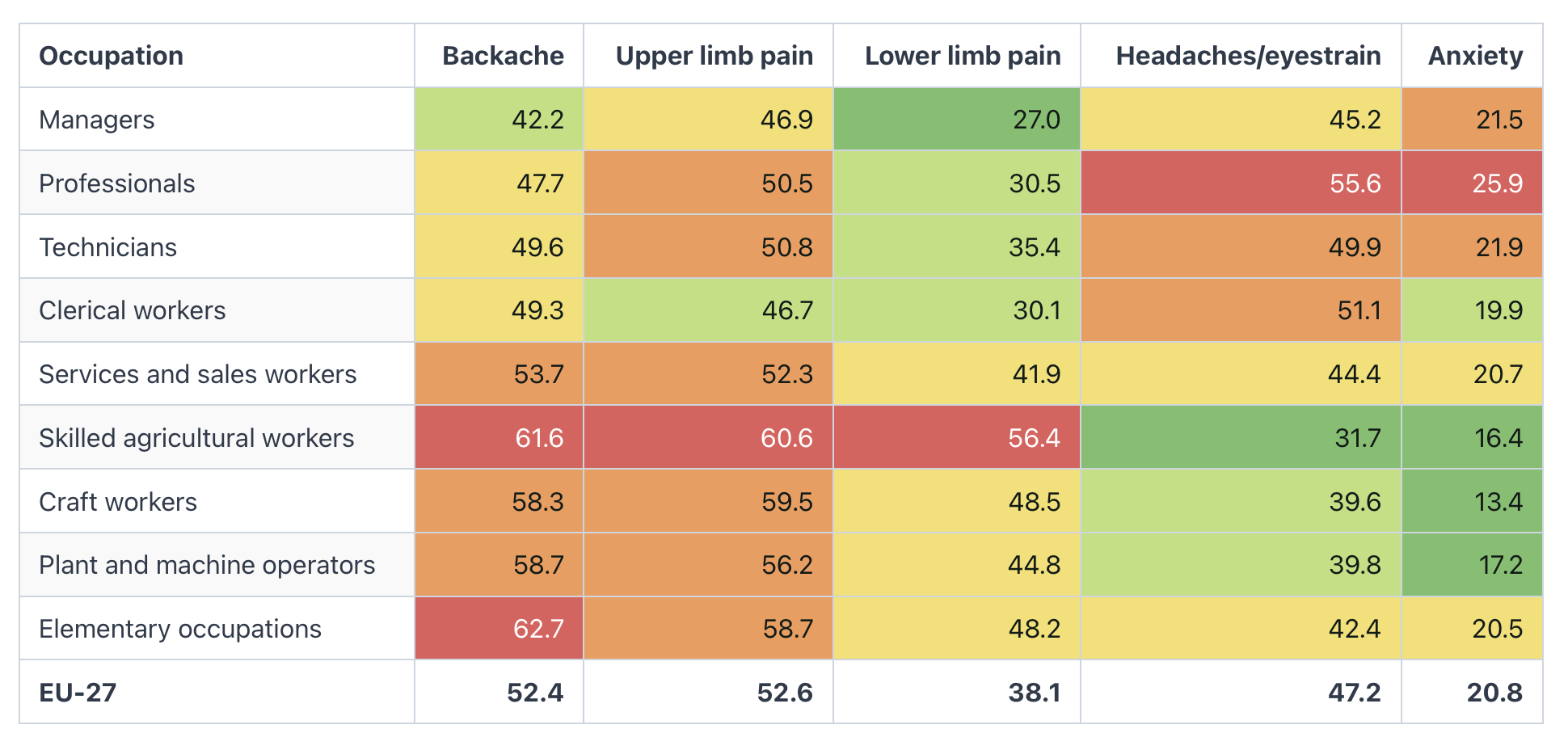
Data from the EU Labour Force Survey (EU-LFS) show that the most common types of work-related health problem are MSDs, which affect 6.0% of all employed or formerly employed people aged 15-64 at EU level[5]. Data from the OSH Pulse survey[6] show that in 2025, 28% of the respondents experienced ‘Bone, joint or muscle problems or pain’ the last 12 months, that were caused or made worse by their work. Only ‘Overall fatigue’ (37%), ‘Headache and eyestrain’ (35%) and ‘Stress, depression or anxiety’ (28%) received higher responses. Low-educated workers are more likely to report 'bone, joint or muscle problems or pain' than higher-educated respondents. Looking at economic sectors, MSDs were most commonly reported in agriculture, horticulture, forestry or fishing (32%), followed by services related to health and social care (31%), and commerce, transport, accommodation or food services (31%)6. Furthermore, data from the European Working Conditions Survey (EWCS, 2024)[7] show that the health problem most reported by workers in 2024 was upper limb pain (reported by 52,6%), followed by backache (52,4%). Muscular pains in the lower limbs are reported by 38,1% (figure 1).
Figure 1: Health problems reported in the 12 months before the survey, EU27 (%) - EWCS, 2024
MSDs represent a significant burden on workers’ health and productivity, and their impact can be measured in terms of disability-adjusted life years (DALYs). DALYs for an illness or health condition are calculated as the sum of the years of life lost due to premature mortality (YLL) in the population and the years lived with disability (YLD) for people living with the health condition or its consequences. In other words, DALYs indicate the gap between current health status and an ideal situation in which individuals live into old age without disease and disability. In 2021, the International Labour Organisation (ILO) and the World Health Organization (WHO) published joint estimates of the work-related burden of diseases and injury for the years 2000-2016[8]. Figure 2 shows the share of total DALYs attributable to the main work-related disease and injuries in DALYs. Cancer accounts for the main part of the cost (35%), and MSDs follow at approximately 20 %. In other words, MSDs represent 20% of the burden of diseases caused by the listed work-related diseases and injuries.
Figure 2: Distribution of the main work-related illnesses work-related diseases by DALYs
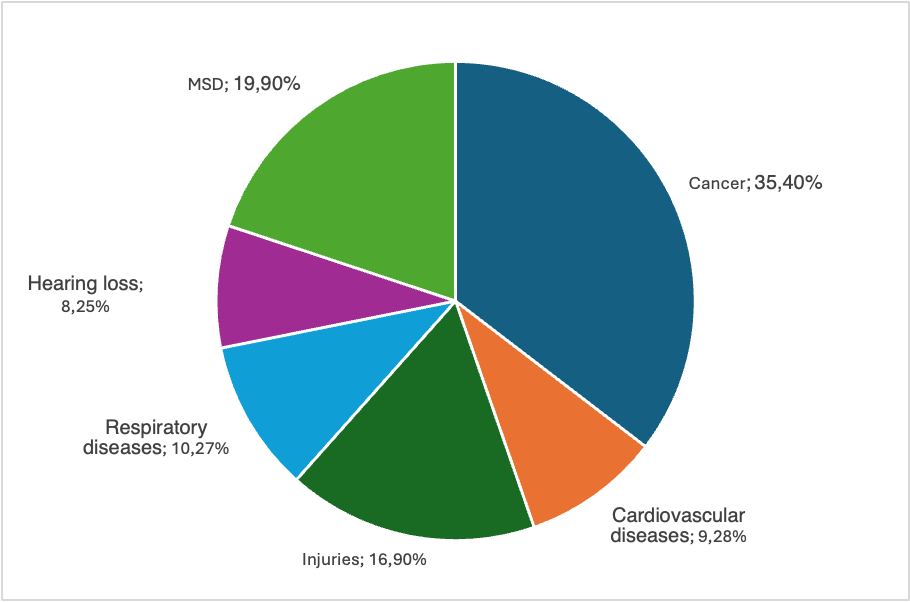
Source[8]
In addition to their contribution to DALYs, MSDs are a major cause of sick leave. According to a report published by Eurostat in 2007, about 60% of all short term (< 1 month) and long term (at least 1 month) sickness absence reported in the previous 12 months can be attributed to musculoskeletal problems[9]. Similarly, data from the EWCS 2015 shows that workers with MSDs tend to be absent from work more often than others. As shown in Figure 3, more than half of the workers with MSDs and other health problems were absent from work for at least 1 day, while around 23 % were absent for at least 10 days – proportions notably higher than those for workers with other health problems or none.
Figure 3: Number of days absent in the past 12 months due to a health problem: distribution of workers, for workers with MSDs and/or other health problems and without health problems, EU-28, 2015
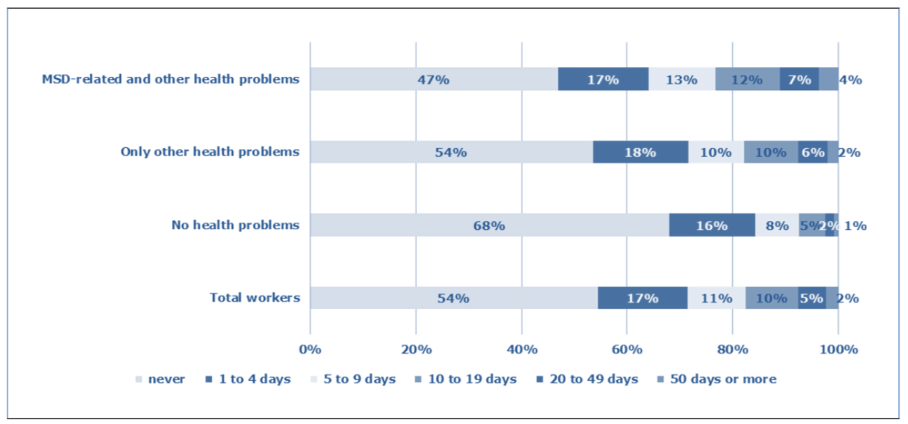
Source: Panteia based on the sixth (2015) wave of the European Working Conditions Survey (EWCS)1
While sickness absence already represents a major economic impact of MSDs, their costs extend to broader losses in productivity and societal expenses. These includes reduced company compensation payments, medical care, and administrative costs. In some EU Member States, MSDs account for around 40% of workers’ compensation expenses, representing up to 1.6% of national GDP[10]. According to BAuA (Federal institute for occupational safety and health - Germany), MSDs rank second only to respiratory diseases in terms of the cost of work-related illnesses. Estimates suggest EUR 21.5 billion in production losses (based on labour costs) and EUR 37.7 billion in lost gross value added (loss of labour productivity) due to MSDs[11].
Work-related MSDs are multifactorial, with numerous risk factors contributing to their development. These includes physical and mechanical factors, organisational and psychosocial factors, as well as individual characteristics. Workers are often exposed to several of these factors simultaneously[12].
With regard to physical risk factors, studies have found reasonable evidence for an association between different types of MSDs and the following physical risk factors[1] [13]:
Data from the European Working Condition Survey (EWCS) show that MSDs are associated with working in tiring or painful positions, carrying or moving heavy loads and repetitive hand or arm movements. This applies to all three types of MSDs that are distinguished in the survey, namely upper limbs, lower limbs and back pain. Other physical risk factors are known to be associated with MSDs, such as vibrations from hand tools and machinery and low temperature. EWCS data from 2005, 2010, and 2015 shows a light decrease in exposure for most of these risk factors (Figure 4). However, European workers remain exposed to physical hazards linked to MSDs: 32% carry heavy loads at least a quarter of their working time, 20% are exposed to vibration, 40% work in tiring or painful postures for at least a quarter of the time, and 61% perform repetitive hand or arm movements[1].
Figure 4: Percentage of workers reporting that they are exposed to different physical risk factors at their work at least a quarter of the time, EU-28, 2005, 2010 and 2015
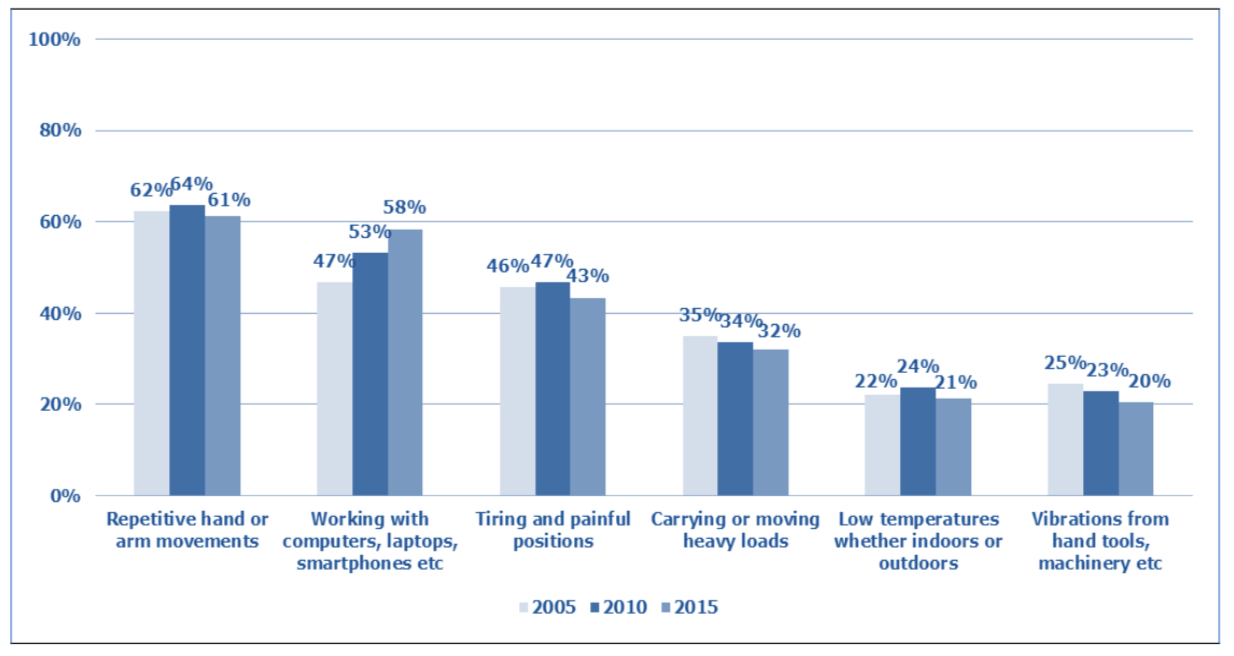
Source: Panteia based on the European Working Conditions Survey (EWCS)1
Psychosocial risks can also contribute to the development of MSDs. An EU-OSHA study (2021)[13] identified several work-related psychosocial factors significantly associated with MSDs:
MSDs are common among workers in sectors such as agriculture, construction, transport, manufacturing, hospitality, and health and social care due to high exposure to physical risk factors.
Women workers are less likely to perform heavy physical work but more often face other physical risk factors such as lifting or moving people, repetitive tasks, awkward postures and prolonged standing or sitting[14]. These factors, combined with psychosocial risks, contribute to the relatively high prevalence of MSDs among women. Although job and sector differences partly explain women’s higher MSD prevalence, some studies indicate that women are more likely than men to report musculoskeletal complaints even when working in the same roles and sectors. Additionally, it has been demonstrated that female workers are at greater risk of developing MSDs when exposed to multiple risk factors, including both physical and psychosocial factors[14].
More information on groups at risk is available in the EU-OSHA report Preventing musculoskeletal disorders in a diverse workforce: risk factors for women, migrants and LGBTI workers[14].
Work-related musculoskeletal disorders (MSDs) can affect different parts of the body, with the lower back, neck, shoulders, and upper limbs being most commonly impacted, while lower limb disorders occur less frequently. The following subsections outline the main types of work-related MSDs by body region and their associated risk factors.
Work-related Upper Limb Disorders (WRULDs) can affect any region of the neck, shoulders, arms, forearms, wrists and hand. Some of WRULDs, such as tendonitis, carpal tunnel syndrome, osteoarthritis, vibration white finger and thoracic outlet syndrome have well-defined signs and symptoms, while others are less well-defined, involving only pain, discomfort, numbness and tingling.
Other, similar terms for WRULDs include[15] [16]:
WRULDs have been associated with physical risk factors such as heavy physical work, prolonged computer work, repetitive work, psychosocial factors and individual characteristics such as a high body mass index1. Prolonged static sitting and the increasing use of digital technology also contribute to the development of WRULDs[1].
The most common WRULDs are:
Low back work-related MSDs include spinal disc problems, muscle and soft tissue injuries. These disorders are mainly associated with physical work, manual handling and vehicle driving activities, where lifting, twisting, bending, static postures, and whole-body vibration are present.
Lower limb MSDs is a problem in many workplaces and they tend to be related with conditions in other areas of the body. Lower Limb Disorders affect the hips, knees and legs and usually happen because of overuse. Workers working over a long period in a standing or kneeling position are most at risk. Work-related lower limb MSDs have been associated with the following physical risk factors[17][18]:
The most common work-related lower limb MSDs are:
Non-specific work-related MSDs are musculoskeletal disorders that have less well-defined symptoms, i.e. the symptoms tend to be diffuse and non-anatomical, spread over many areas: nerves, tendons and other anatomical structures[19]. The symptoms involve pain (which becomes worse with activity), discomfort, numbness and tingling without evidence of any discrete pathological condition.
The table below summarises the main MSDs described above and groups them according to the part of the body and anatomical structure affected.
Table: Main MSDs according to the body part and anatomical structure affected
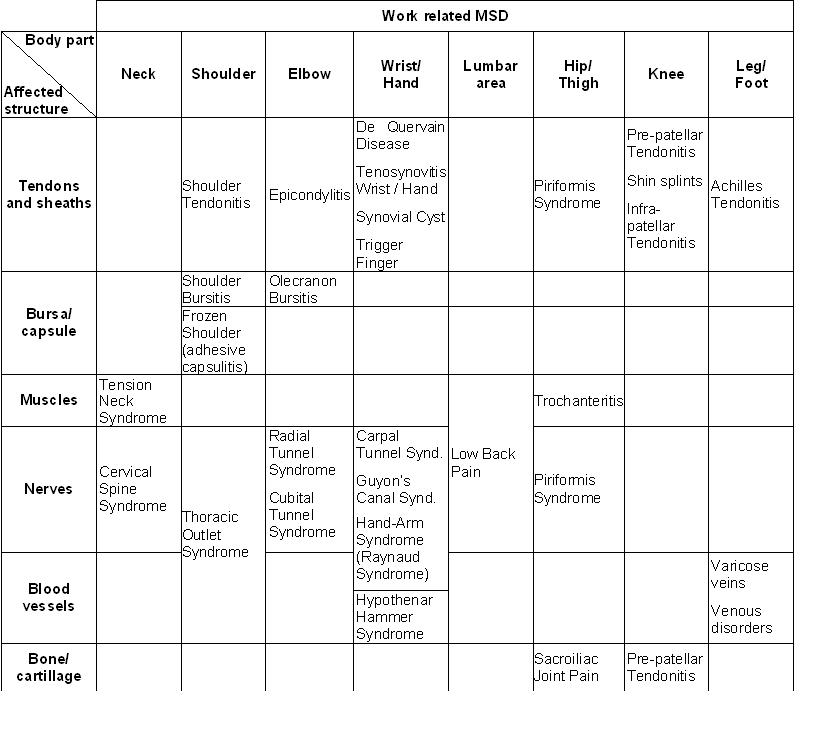
Source: adapted from[15] and [20]
[1] EU-OSHA – European Agency for Safety and Health at Work, Work-related musculoskeletal disorders: prevalence, costs and demographics in the EU, 2019. Available at: https://osha.europa.eu/en/publications/msds-facts-and-figures-overview-prevalence-costs-and-demographics-msds-europe/view
[2] EU-OSHA – European Agency for Safety and Health at Work. Musculoskeletal disorders. Available at: https://osha.europa.eu/en/themes/musculoskeletal-disorders
[3] Putz-Anderson, V., Cumulative Trauma Disorders: A Manual for Musculoskeletal Diseases of the Upper Limbs, Taylor & Francis, 1988
[4] Nunes, I. L., 'FAST ERGO_X – a tool for ergonomic auditing and work-related musculoskeletal disorders prevention', ''WORK: A Journal of Prevention, Assessment, & Rehabilitation'', 34, 2009, pp.133-148
[5] Eurostat. Self-reported work-related health problems and risk factors - key statistics. Statistics explained, 2021. Available at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Self-reported_work-related_health_problems_and_risk_factors_-_key_statistics
[6] EU-OSHA – European Agency for Safety and Health at Work. OSH Pulse 2025: Occupational safety and health in the era of climate and digital change Report, 2025. Available at: https://osha.europa.eu/en/publications/osh-pulse-2025-occupational-safety-and-health-era-climate-and-digital-change
[7] Eurofound (2025), European Working Conditions Survey 2024: First findings, Publications Office of the European Union, Luxembourg.. Available at: https://www.eurofound.europa.eu/en/publications/all/european-working-conditions-survey-2024-first-findings
[8] WHO/ILO joint estimates of the work-related burden of disease and injury, 2000-2016: Global monitoring report: Geneva: World Health Organization and the International Labour Organization, 2021. Licence: CC BY-NC-SA 3.0 IGO 6. Available at: https://www.who.int/publications-detail-redirect/9789240034945
[9] Eurostat. Health and safety at work in Europe (1999-2007) – A statistical portrait, Inna Šteinbuka, Anne Clemenceau, Bart De Norre, August 2010. Available at: http://ec.europa.eu/eurostat/en/web/products-statistical-books/-/KS-31-09-290
[10] EU-OSHA – European Agency for Safety and Health at Work, Work-related musculoskeletal disorders: Back to work report, 2007. Available at: https://osha.europa.eu/en/publications/report-work-related-musculoskeletal-disorders-back-work
[11] Federal Institute for Occupational Safety and Health (BAuA), Arbeitswelt im Wandel: Zahlen — Daten — Fakten (Changing working world: facts and figures), 2024. Available at: https://www.baua.de/DE/Angebote/Publikationen/Praxis/A113
[12] INRS. TMS Troubles musculosquelettiques. Facteurs de risque. Available at: https://www.inrs.fr/risques/tms-troubles-musculosquelettiques/facteurs-risque.html
[13] EU-OSHA – European Agency for Safety and Health at Work. Musculoskeletal disorders: association with psychosocial risk factors at work. Report, 2021. Available at: https://osha.europa.eu/en/publications/musculoskeletal-disorders-association-psychosocial-risk-factors-work
[14] EU-OSHA – European Agency for Safety and Health at Work. Preventing musculoskeletal disorders in a diverse workforce: risk factors for women, migrants and LGBTI workers. Report, 2020. Available at: https://osha.europa.eu/en/publications/preventing-musculoskeletal-disorders-diverse-workforce-risk-factors-women-migrants-and
[15] Nunes, I. L., Modelo de Sistema Pericial Difuso para Apoio à Análise Ergonómica de Postos de Trabalho [Fuzzy Expert System Model to Support Workstation Ergonomic Analysis], Dep Eng Mecânica e Industrial, Universidade Nova de Lisboa, Lisbon, Portugal, 2003
[16] van Tulder, M., Malmivaara, A., Koes B., Repetitive strain injury, Lancet, 2007; 369, pp.1815-22, Available at: http://www.ncbi.nlm.nih.gov/pubmed/17531890
[17] HSE - Health and Safety Executive, Lower Limb disorders. Available at: http://www.hse.gov.uk/msd/lld/index.htm
[18] Santos, C., Gabriel, A. T., Quaresma, C., & Nunes, I. L. (2023). Risk factors for lower limb work-related musculoskeletal disorders. In Occupational and Environmental Safety and Health V (pp. 187-203). Cham: Springer Nature Switzerland.
[19] Ring, D., Kadzielski, J., Malhotra, L., Lee, S.-G. P. & Jupiter, J. B., Psychological Factors Associated with Idiopathic Arm Pain, The Journal of Bone and Joint Surgery (American), 87, 2005, pp. 374-80.
[20] EU-OSHA – European Agency for Safety and Health at Work. Work-related neck and upper limb musculoskeletal disorders. Report, 1999. Available at: https://osha.europa.eu/en/publications/report-work-related-neck-and-upper-limb-musculoskeletal-disorders
EU-OSHA - European Agency for Safety and Health at Work. Practical tools and guidance on musculoskeletal disorders, Available at: https://osha.europa.eu/en/themes/musculoskeletal-disorders/practical-tools-musculoskeletal-disorders
EU-OSHA - European Agency for Safety and Health at Work. Healthy workers, thriving companies - a practical guide to wellbeing at work. Guide, 2018.Available at: https://osha.europa.eu/en/publications/healthy-workers-thriving-companies-practical-guide-wellbeing-work
EU-OSHA - European Agency for Safety and Health at Work, Conversation starters for workplace discussions about musculoskeletal disorders. Training resource, 2019. Available at: https://osha.europa.eu/en/publications/conversation-starters-workplace-discussions-about-musculoskeletal-disorders
EU-OSHA – European Agency for Safety and Health at Work. Work-related musculoskeletal disorders: prevalence, costs and demographics in the EU. Report, 2019. Available at: https://osha.europa.eu/en/publications/msds-facts-and-figures-overview-prevalence-costs-and-demographics-msds-europe/view
EU-OSHA – European Agency for Safety and Health at Work. Work-related musculoskeletal disorders: why are they still so prevalent? Evidence from a literature review. Report, 2020. Available at: https://osha.europa.eu/en/publications/work-related-musculoskeletal-disorders-why-are-they-still-so-prevalent-evidence-literature-review
EU-OSHA – European Agency for Safety and Health at Work. Musculoskeletal disorders: association with psychosocial risk factors at work. Report, 2021. Available at: https://osha.europa.eu/en/publications/musculoskeletal-disorders-association-psychosocial-risk-factors-work
Selectați tema