

Emergency workers are people, who work in emergency response situations, such as fire-fighters, paramedics and police officers. Their specific work demands can be divided into physical, mental and environmental or task-defined. Time pressure, significant physical and psychological stress and unpredictable, rapidly changing work conditions increase stress and create special characteristics of the demands of the work in emergency situations. Important OSH issues are accidents, work-related diseases and symptoms, work ability and ageing-related issues.
Emergency workers work in emergency response situations protecting human life, property and the environment during accidents and major incidents and disasters. More specifically these professionals provide assistance and support in critical situations, such as medical emergencies, fire, natural disasters, incidents and rescue situations. Professional categories that fall under this umbrella include paramedics, police officers, firefighters, disaster recovery workers and support personnel[1]. In emergency situations, more than one professional group might be involved depending on the extent and consequences of the incident. It is difficult to define the exact numbers of European emergency workers even for the everyday work situations, and especially for major incidents. According to Eurostat, for example, there were 362,400 professional firefighters in the EU in 2023, representing 0.18% of the total EU employment. The number of firefighters increased by 3,200 compared with 2022[2]. In addition to workers with a permanent contract, there are many part-time and voluntary emergency workers. The article focuses mainly on permanent fire-fighters, police officers, paramedics and to some extent on special forces for disaster control, e.g. military forces, mostly emphasising the OSH issues encountered in (every day) emergency situations.
In emergency situations, the physical work demands imposed on fire-fighters, paramedics and police officers are high, versatile and task specific. Apart from work equipment and procedures, it is almost impossible to influence the physical exposure during emergency situations. Typical fire and rescue tasks, such as working in smoke-filled or hazardous gas environments, roof work and handling patients, victims or heavy tools, require a high level of physical ability to ensure they are carried out safely and effectively[3] [4]. Temporary thermal and ground conditions, and the use of protective equipment further increase the demands on the cardiorespiratory and musculoskeletal systems, as does the requirement for postural and movement control[5][6]. The typical physical work demands to be met by police officers involve sudden and occasional very severe physical efforts e.g. in chasing and tackling suspects and between these kinds of operations, there are long inactive periods[7].
The dynamic stress imposed on the emergency workers can be assessed via the measurement of oxygen consumption during work. Depending on the task and the environmental demands, the average body oxygen consumption in simulated smoke-diving[i] ranges between 31–44 and ml/kg/min[3] [8] [9], and between 18–40 ml/kg/min in ambulance service and first aid tasks[10] [11]. A systematic review of the metabolic demands of firefighting tasks[12] found similar results, demonstrating that firefighters may work at an intensity of up to 40 ml/kg/min while wearing a firefighting ensemble during simulations. The mean oxygen consumption of the correctional officers while they were responding to an incident and then controlling and restraining inmates was 39 ml/kg/min [13]. The body's oxygen consumption at rest is 3,5 ml/kg/min, 14 in walking at 4 km/h and 35 when jogging at 10 km/h. Light office work demands 5 and cleaning work 12 ml/kg/min of body's oxygen consumption. The higher the demand of oxygen consumption of the work, the higher is the strain imposed on the worker. Therefore, it is important that emergency workers maintain sufficient fitness in accordance with their work demands.
Furthermore, working with heavy tools, rescuing and carrying patients and victims and working at height demand a great deal of muscular strength and endurance as well as balance and agility. For example, the opening of a ceiling with a motor saw in simulated fire-fighting, the compressive force exerted on the low back was found to be so high that the risk for back injuries increased considerably[4]. According to Lavender[14], the most demanding tasks requiring muscular strength as well as hazardous tasks for the low back involved moving a victim from a bed to a stretcher, descending of a set of stairs with the stretcher, and lifting a victim off the floor. On average, male correctional officers needed 60 kg force in body control, 49 kg in wrist hold and 47 kg in arm retraction to control and restrain on inmates[13] .
In actual emergency work situations, the contact surfaces are frequently unstable, narrow, inclined or slippery. Workers may have to climb ladders, work on roofs or work in moving emergency vehicles. Sometimes the environment is smoky, dim or completely dark. Then the visual feedback will be poor. All these aspects pose major challenges on the postural control system. First aid tasks and the use of different tools also require good hand-eye coordination and motor coordination of fingers.
Due to these high and versatile physical work demands, it is important to systematically follow-up the physical work capacity of emergency workers.
Emergency workers are regularly exposed to traumatic events, including life-threatening situations, severe injuries and deaths of colleagues and civilians[15]. Studies reveal that they are at a heightened risk for conditions like Post-Traumatic Stress Disorder (PTSD), depression and anxiety[16]. Furthermore emergency workers are exposed to both physical and verbal violence from third parties such as patients or bystanders[17].
Their work often involves irregular and long working hours, sometimes up to 24 hours at a time, as well as night and shift work. Many work tasks have to be done under intense time pressure and the stressful nature of these situations can provoke anxiety and increase the risk of errors. Emergency workers must be able to make quick and critical decisions, rely on their co-workers and always be aware that they may be in life-threatening situations themselves. Mental stress increases also during major incidents, such as shootings or a bomb attacks[18], which often attract public and media attention.
Mental stress can also be attributed to poor management especially in operational situations involving teams from different disciplines at the same time. There may be incorrect or incomplete information, traffic congestion, lack of protective equipments or other necessary resources as well as lack of social support or psychosocial assistance after major incidents. One risk factor for emergency workers, especially for paramedics, which seem to be associated with burnout, is the requirement to suppress their own emotions at work but at the same time to be emotionally empathetic[19]. Incidents that involve children, suicides, or traumatic amputation are considered as the most distressing for ambulance personnel[20].
Disasters can be categorised into four main groups: (1) disasters of natural origin (e.g. floods, seismic events, hurricanes, forest fires), (2) disasters caused by industrial accidents (e.g. nuclear accidents, release of chemicals, mining accidents), (3) disasters caused by transport accidents (e.g. major car crashes, airplane crashes, rail accidents), and (4) disasters caused by terrorist or criminal attacks and any combination of these four groups. Emergency aid and disaster control are mentally and physical extremely challenging and demanding tasks.
Environmental problems can be caused by weather conditions (rain, snow, heavy wind, bright lights, and heat), the time of day (night, dawn), and the place where the disaster strikes. These can pose specific OSH risks to emergency workers and complicate their mission. There are different types of environmental work risks e.g. chemical emissions (carbon monoxide, loss of oxygen, impurities etc.), extreme thermal conditions (cold, heat), risk of drowning or radiation (ionising, optical and non-ionising), noise and vibration. The Infrastructure and its related systems can be destroyed and emergency workers must work inside ruined buildings.
Working in confined spaces is also a very common scenario for rescue workers in all forms of natural disasters. Fire-fighters, employees of relief organisations or soldiers often have to clear various layers of debris in order to reach the victims, and on occasions it may even be necessary for them to enter the confined spaces in which the victims are themselves entrapped. Vegetation fires put emergency workers at risk from strong smoke development and OSH risks posed by wild or domestic animals. Landslides and earthquakes cause dust production. All those factors (ash, gases, smoke, and dust) together can cause many kinds of irritative and subsequent health effects.
Emergency workers have to respond to serious incidents in industrial installations such as toxic releases or major fires or explosions in manufacturing plants or mines when flammable and/or explosive substances are present. Explosions can also be caused by physical processes e.g. if the energy present in compressed gas or vapour is suddenly liberated (vessel explosions).
An explosion is a sudden and violent release of energy that causes a blast. Energy can be released as physical, chemical and nuclear energy. Physical energy for example can be released when a vessel containing a high pressure gas is suddenly ruptured. Chemical explosions related to chemical reactions are of major importance for studying major accidents involving hazardous materials. Explosion related to the combustion of flammable gases can be either “deflagration" or “detonation" depending on the burning velocity. For example Industrial installations that can potentially create a major accident are: chemical and petrochemical industries, oil refineries, storage of gas and flammable liquids, chemical warehouses, fertiliser manufacturing plants, water treatment works using chlorine, and mines[21].
The increasing density of transportation routes also increases the probability of small-scale emergencies and disasters during transport. This also enhances the probability of emergency workers being deployed to deal with transport disasters. The hazards to which emergency workers are exposed in transport accident scenes can vary greatly depending on the type of transport, the products being transported, and the location of the accident. In transport accidents, it is not always possible to undertake an appropriate assessment of the risks, because not all risks are immediately visible. The incident combines different elements that need to be taken into account: search for victims, risks of fire and explosions, presence of hazardous material, heavy equipment, water rescue, extrication and multiple casualties.
Emergency work poses many risks resulting in accidents and work-related diseases and symptoms throughout their work career. These negative outcomes can lead to reduced work ability, sick absence and early retirement.
Emergency workers often have to work in unpredictable, dynamic and hazardous environments which makes them vulnerable to various types of accidents. Even a minor accident can require an emergency worker to take sick leave because of the heavy physical demands of the job. In the long run, if not rehabilitated properly, accidents often lead to musculoskeletal problems and carry the possibility of early retirement.
The most frequent non-fatal accidents suffered by emergency workers are injuries while handling, lifting and carrying or moving equipment, people or vehicles associated with physical overstrain (20-41%). Slips, trips or falls on the same level (14-28%) were the secondly frequent accidents followed by being hit by a moving, flying or falling object or being trapped between objects and equipment (6-9%). The most prevalent injuries were muscle and tendon strains and sprains and dislocations. Wounds, laceration and other superficial injuries are the second most common injuries. The back, lower and upper extremities were the body parts most often injured[22] [23].
A considerable number of injuries happen during training at work and free time. According to Konttinen et al[7], only 38% of all accidents in police officers were work-related with 51% being associated with physical exercise. A further 33-38% of all accidents were due training at work. There are several other studies from Sweden, Poland, Finland and Germany revealing that on-duty fitness training has been responsible for injuries to fire-fighters and police officers. The proportion of injuries due by physical training ranges from 25 to 50% of all accidents[22] [23].
Emergency workers also suffer the risk of assaults and injuries by violent or combative patients[23]. For example, in Sweden 80% of emergency paramedics had been threatened or subjected violence, 67% subjected to physical violence, and over one third had experienced threats of violence every 3 months, usually from a patient, a relative or a friend of the patient. Similar results about the prevalence of violence targeted at Finnish emergency workers have been reported: 73% of them had been threatened or been targets of violence. Moreover, in Finland, 14% of police officers' and 2% of fire-fighters' injuries were attributed to shock, violence, aggression, etc. In France, 23% of the ambulance personnel have experienced one or more assaults during their careers, of which 4% resulted in sick leave[22].
Work-related diseases and symptoms can be divided into musculoskeletal disorders (MSDs), and health outcomes resulting from psychosocial risks, chemical or biological risks, or exposure to radiation.
The genesis of MSDs is multifactorial and occurs as a consequence of exposure to many stressors observed in the emergency work[24][25] [26] [27]. The risks for MSDs among emergency workers are physical (high physical work load, sedentary activity, whole-body vibrations, for example related to driving large vehicles etc.) as well as psychological. Most frequently the back, neck, shoulders, upper limbs (including shoulders, arms, hands and wrists) although in fire-fighters knees are also affected. A systematic review[28] found that, although there's considerable variation between different studies, on average, 56.5% of emergency medical personnel experience MSDs. The areas most affected are the lower and upper back, shoulders and neck[28].
MSDs have been proved to be the leading cause for early retirement in many countries. Furthermore, psychological overload can increase the risk for MSDs, especially those related to major disasters. For example Morren et al[29] claimed that cases of MSDs increased among fire-fighters, police officers and emergency service personnel involved in an explosion of a fireworks depot in the Netherlands in 2000. This was confirmed by the results of Berrios-Torres et al[30], who studied rescue workers who worked in New York during the 11 September 2001 disaster.
The consequences of exposure to traumatising situations can range from stress reactions to more severe consequences like PTSD, burnout and depression. Most emergency workers experience stress reactions during and after a traumatic event. These reactions can include emotional reactions (e.g. shock, anger, and helplessness), cognitive reactions (e.g. disorientation, memory loss, guilt), physical reactions (e.g. tension, fatigue, pain, elevated heart rate) and psychosocial reactions (e.g. isolation, distrust, becoming distant)[31]. Some workers have a higher risk of developing more serious psychological problems due to their experiences of prior events or during the actual event. Many studies indicate that emergency workers are at a higher risk of developing PTSD, even if they are not exposed to major disasters [32]. The symptoms of PTSD are persistent re-experiences, intense psychological distress and increased arousal (e.g. concentration problems). The most important characteristics of burn-out are exhaustion together with tension complaints, reduced efficiency or motivation, problematic attitudes and behaviour characteristics. Depression is a complex mental disorder that can manifest in various forms. The most common type is characterised by a major depressive episode involving symptoms such as a depressed mood and a loss of interest in daily activities. The study of Bennett et al.[33] found that 10% of the ambulance drivers reported clinical levels of depression.
Emergency workers are often exposed to chemical substances during major accidents but also in everyday life. The main pathways by which these agents enter the body are via skin, airways or digestive tract. Their effects can appear immediately (e.g. irritation of eyes) or be delayed (e.g. cancer). Exposure to chemicals can lead to acute as well as chronic effects. The International Agency for Research on Cancer (IARC) has classified occupational exposure as a firefighter as carcinogenic to humans (group 1)[34].
Emergency workers might come into contact with blood or body fluids from other individuals and therefore face the risk of transmission of blood-borne diseases. Three main diseases are of concern: HIV, hepatitis B and hepatitis C[35]. Transmission of hepatitis B and C is mostly the result of needle stick injuries[36]. During disasters, where rescuers from many countries are working together, water- and vector-borne diseases might also be a risk e.g. cholera or malaria. With respect to air-borne diseases also tuberculosis can be a risk in regions where it is prevalent. In extreme situations rescuers might become victims of bioterrorism, release of e.g. smallpox.
There are many demands associated with the work ability of emergency workers. The concept of work ability is multidimensional making it difficult to operationalise. Therefore there are few valid methods for measuring work ability. The holistic approach of work ability involves assessing individual resources, work-related factors and the environment outside work[37]. A questionnaire-based measure, the work ability index (WAI)[38][39] has been devised to operationalise the concept of work ability. The WAI is a sum variable which reflects perceived work ability and number of diseases. The Work ability index has four categories: excellent, good, moderate and poor. When WAI is good or excellent, it is important to support and maintain work ability. For those individuals whose WAI is moderate, measures to help improve work ability are recommended. Measures directed toward restoring work ability or additional evaluations of work ability are needed by those whose WAI is poor. WAI can be used as one of the methods for assessing work ability in health examinations, workplace surveys and it can be used in Workplace Health Promotion programmes. Especially among middle-aged and older workers, the WAI can also be used for early detection of a decline in work ability. The Index is in use in several countries in Europe and other countries, and it has been translated in over 30 languages[40].
Among different aged Finnish police officers in 2011 (mean age 38 and 49 years), the WAI can be classified as good[7] [41]. In fire-fighters with a mean age of 36 years the WAI was also good but after 13 years follow-up their average WAI had decreased to moderate[42]. The mean value of WAI among paramedics aged 36 years (21-56 years) was also good[10]. However, although the mean WAI value for emergency workers was mostly good, it was poor or moderate in 3 to 15% of the subjects, which poses a risk of disability[43][41] so actions for restoring and improving work ability are needed.
Age is strongly associated with WAI. For example, in fire-fighters with a 13-years follow-up, the risk for poor work ability in fire-fighters over 45 years was as elevated as seven-fold compared to those under 30[44]. In addition to age, individual life style factors were very powerful risk factors in fire-fighters in a three-year follow-up, but no longer after a 13-year follow-up. Factors related to work skills and the organisation of work were emphasised in both time periods. The significance of those factors related to leadership even increased with the longer follow-up time period. Life dissatisfaction and lack of positive feedback regarding work were also associated with WAI[44].
In police officers and fire-fighters, good physical capacity was significantly associated with good WAI[45][7][42]. Moreover, good muscular capacity was a protective factor whereas poor motor control was a risk factor for reduced perceived physical work ability in relation to the physical demands of the fire and rescue work[42]. It is the responsibility of every emergency worker as well as his/her superiors and management in the workplace to maintain and support the individual's work ability.
Europe’s population is becoming progressively older. The proportion of people aged 55 and over increased from 25% in 1990 to 30% in 2010[46] and 38% in 2022[47]. Furthermore, the share of the working-age population is expected to continue declining, while older people are likely to account for an increasing proportion of the total population. By 2100, those aged 65 years or over are expected to account for 31.3% of the EU’s population, compared with 21.1% in 2022[48].
These scenarios pose challenges for emergency workers. Not only will they themselves be older, but also the people they rescue will be older.
The relationship between aging and work ability is complex. The diversity of the various demands (i.e. physical, mental or psychosocial) to which the emergency workers need to respond needs to be considered in any assessment of work ability[49]. According to the meta-analysis conducted by Sehl and Yates[50] the capacity of the different physiological systems declines by between 0.3-1.3% per year and the loss rates in integrative tasks, requiring interaction and function of almost all organ systems on average linear decline were by 0.97% per year. The most robust decline in cognitive human functions is thought to occur in general slowness (other functions are reaction time, memory and decision-making), whereas intellectual abilities do not appear to change with aging. Although there are general estimates for the rates at which ageing affects specific bodily systems and capacities, information is lacking on the extent to which these indices correlate with real work ability. Furthermore, general population data may not reveal valid data to be extrapolated to high-demand jobs, such as emergency work. Older emergency workers have longer work experience for example they have better work techniques and greater ability to cope with demanding work situations than younger workers. The main goals should be to keep ageing workers healthy in their jobs, increase the safety of (co)workers and optimise the worker-job interaction[49].
Occupational health and safety (OSH) management should be performed systematically as part of normal daily routines and management. Implementing an OSH management system as a part of company practice is essential for enhancing the health and safety of workers. Employers have the responsibility in co-operation with OSH personnel to create conditions that protect emergency workers from adverse health outcomes.
The risks in emergency work are not only serious but also multiple. They can cause major injuries and health problems. In addition to the traditional risks, emergency workers can encounter new risks, such as technological disruptions hindering communication. Therefore efficient risk management is vital (Figure 1). The risk management process at a scene of a major incident can be divided into three steps: information gathering, analysing alternative options for action and decision making and taking action[51] .
In all emergency situations, the key to protecting the health and safety of workers is planning and preparedness[52]. It has been suggested that highly trained emergency workers experience a lower prevalence of psychological problems following disasters than their less trained colleagues[53]. Experience and preparedness can reduce the stress faced by emergency workers in disaster situations[54] and therefore emergency workers should also be trained and prepared for different types of major incidents[55]. In addition, organisations need to undertake joint drills, and they should also be prepared to cope with intense media interest surrounding major incidents. It has been stated that strategic planning and implementation of standardised systems and procedures that have been tested beforehand enhance the probability of successful disaster control[51].
Figure 1: Managing risks in emergency work
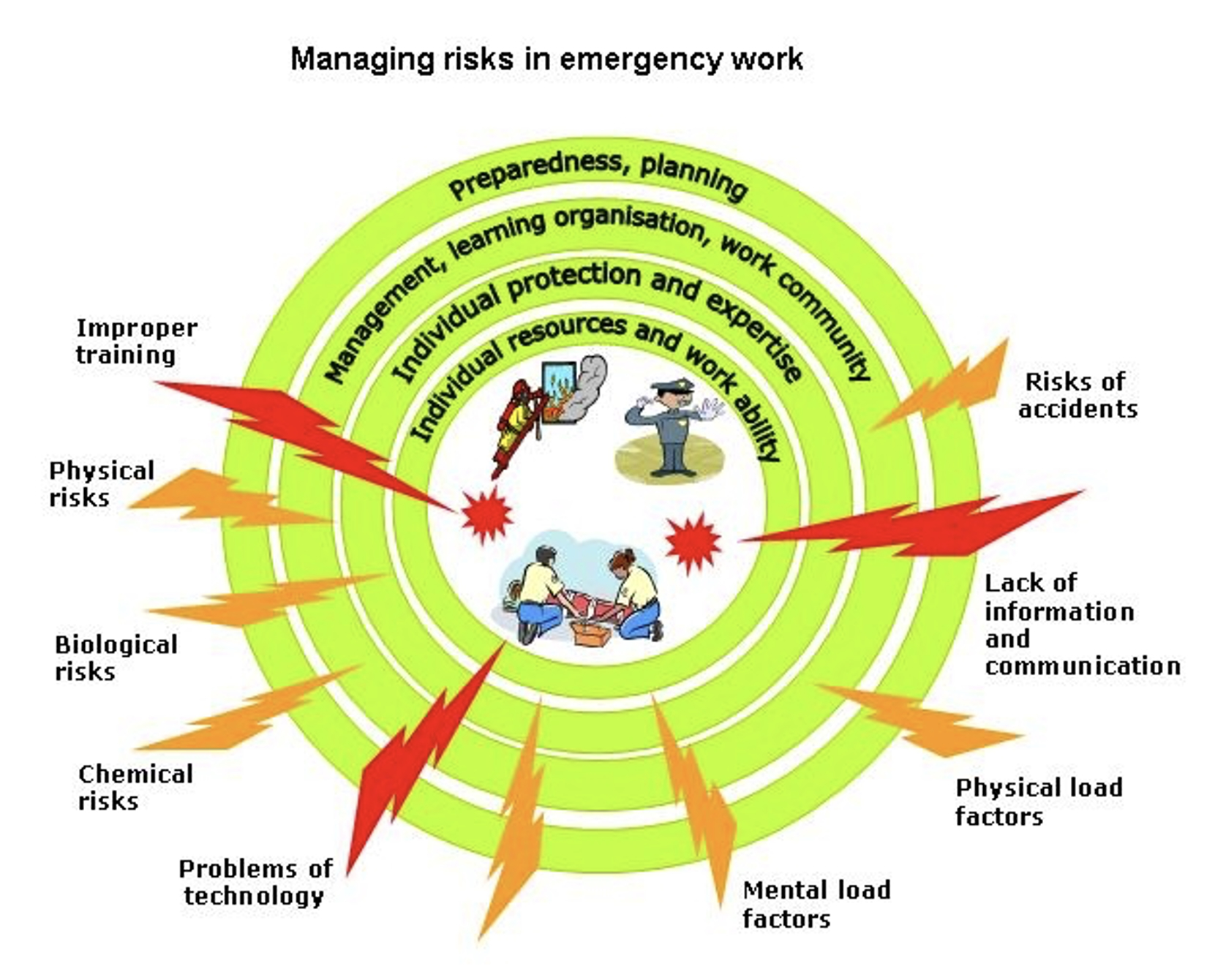
Source: Drawn by the authors
An important managerial issue is how best to provide relevant training and education in order to ensure that expertise and knowledge of emergency workers is up to date. It is important that there is shared responsibility between the individual and the management and work community on this issue. The use of appropriate protective equipment is essential for protection against chemical, biological and physical risks. The PPE must be selected according to the type of intervention and typical work tasks of each group of emergency workers[23]. Good protection is needed against thermal risks, exposure to chemical releases or radiation.
Vaccination should be provided where emergency workers might be at risks of hepatitis B, water-borne diseases or exposed to some biological agents that may be used in bioterrorism.
Social support during and after deployment in a disaster and providing psychological long-term care after the disaster are important preventive measures. However, emergency workers should be provided with primary and secondary prevention from mental problems emerging not only after major disasters but also those related to everyday work. These activities include psychological preparedness, post-intervention psychological support and help, and also long-term psychological care when needed[23].
Maintaining a sufficient level of health and physical capabilities in relation to emergency work demands represent the foundation for good work ability. Good work ability and individual resources can help emergency workers to manage risks, which they face in their daily work. Regular health examinations and physical fitness testing with individualised exercise prescriptions are important preventive factors to combat the decline in work ability. Attention should be paid to exercise, smoking and drinking habits and adopting a healthy lifestyle in general. Employers can help emergency workers to stay in good health and maintain their work ability e.g. by Workplace Health Promotion programmes.
Since emergency workers are especially prone to injuries in the back and lower limbs due to physical overexertion and slipping accidents, it is essential to utilise ergonomic devices and to provide lifting training.
Excellent co-operation between emergency workers is vital for every kind of major incident. The co-operation must be coordinated not only between national, regional and local emergency forces but also between the different occupational groups of emergency workers. Successful co-operation requires training between emergency workers and efficient action within remits must be trained.
A lack of information or only partial availability of information regarding the conditions at the incident site may lead to severe accidents in emergency workers and also victims. Appropriate help can also be given to victims only if information on their situation and condition is properly passed along the chain of command.
Reliable information is necessary to ensure efficient and resource-conserving coordination of the taskforces and to protect them in the best way possible. Therefore emergency plans including alarm and information systems must be devised for different kinds of disasters at regional, state, country, European and international level with responsibilities being clearly defined and allocated before a disaster strikes.
There are several critical areas of protection of safety and health of emergency workers i.e. management, co-operation and communication, protection, training, and physical work capacity. In the future, the work and development of OSH activities of emergency workers will face new challenges.
Increased energy use, dispersion of industrialisation around the globe, expansion of transportation systems, global warming, increased pollution, continuous population growth, and national and international terrorism are only some of the underlying phenomena that may increase the frequency and intensity with which disasters strike as well as the vulnerability of the population to disasters. Major disasters will always occur in addition to the daily emergencies that emergency workers need to face.
Emergency workers often lack sufficient knowledge about the hazards they may encounter. Hence, in the future, their vocational education should focus even more on risk awareness, risk assessment and empowerment. Emergency workers should have some knowledge about the properties of hazardous chemical substances and their effects and they should be able to understand hazardous material symbols. This is particularly important to ensure OSH of emergency workers in case of industrial accidents and accidents in the transportation of dangerous goods.
Future disaster situations must also be anticipated so that appropriate protection equipment (PPE) will be available. In addition to an improved availability of PPE, it is necessary to increase the knowledge of managers, OSH specialists and emergency workers about what PPE to choose in which emergency situation.
The population of EU is ageing and emergency workers are also becoming older. There are also financial reasons to strive to prolong working careers. In high-demanding physical jobs, this can be very challenging. In fact, chronological age should not be the only criterion determining how well an individual can cope with work demands.Because of individual differences in capacities, functional and biological age should also be taken into account. For example this might involve developing functional tests for job-specific work ability. By applying these kinds of tests, individual functional ageing could be monitored and well-timed interventions planned so that workers should be able to work for longer[49]. Work ability issues should be a focus during the whole work career of emergency workers, starting from recruiting methods/criteria to conduct certain activities, followed by interventions during the training and finally in different phases at work. Elderly rescuers can also suffer from illnesses that can limit their possibilities to work in the field; for these individuals retraining possibilities should be available.
Emergency workers are experts in disaster control and vital for a community in the process of returning to normality after a disaster. Moreover, awareness should be raised on the increasing demands imposed on emergency workers as disasters will be more severe in the future and will occur with increased frequency.
[i] Entering smoke-filled environments using self-contained breathing apparatus (SCBA) to search, rescue and extinguish fires.
[1] Bevan, M. P., Priest, S. J., Plume, R. C., & Wilson, E. E. (2022). Emergency first responders and professional wellbeing: A qualitative systematic review. International journal of environmental research and public health, 19(22), 14649.
[2] Eurostat. EU relies on over 360 000 professional firefighters. News article, 23 August 2024. Available at: https://ec.europa.eu/eurostat/web/products-eurostat-news/w/ddn-20240823-1
[3] Holmér, I., Gavhed, D., Classification of metabolic and respiratory demands in fire fighting activity with extreme workloads, Appl Ergon, Vol 38, 2007, pp. 45-52.
[4] Lusa, S., Job demands and assessment of the physical work capacity of fire fighters, Studies in sport, physical education and health 33. University of Jyväskylä Jyväskylä, 1994.
[5] Barr, D., Gregson, W., Reilly, T., The thermal ergonomics of firefighting reviewed, Applied Ergonomics, 2010, Vol 41, pp. 161-172.
[6] Punakallio, A., Lusa, S., Luukkonen, R., Protective equipment affects balance abilities differently in younger and older firefighters, Aviat Space Environ Med. No 74, 2003; pp. 1151-6.
[7] Konttinen, J., Halonen, J., Niemi, J., Lindholm, H., Luukkonen, R., Toivonen, R.,Lusa, S., Poliisien fyysisen toimintakyvyn arviointi ja kuntotestauskäytännöt -kehittämishankkeen loppuraportti. Poliisihallituksen julkaisusarja 1, Helsinki, 2011. (in Finnish).
[8] Lusa, S., Louhevaara, V., Smolander, J., Kivimäki, M., Korhonen, O., Physiological responses of firefighting students during simulated smoke-diving in the heat, Am Ind Hyg Assoc J., Vol 54, 1993, pp. 228-231.
[9] von Heimburg, E., Rasmussen, A., Modbø, J., Physiological responses of fire fighters and performance predictors during a simulated rescue of hospital patients, Ergonomics Vol 49 , 2006, pp.111-126.
[10] Vehmasvaara, P., Ensihoitotyön fyysinen kuormittavuus ja ensihoitajien työkyvyn fyysisiä edellytyksiä arvioivan testistön kehittäminen, Kuopion yliopiston julkaisuja D. Lääketiede, 324, 2004. (in Finnish).
[11] Rice, V.J.B., Sharp, M.A., Tharion, W.J., Williamson, T.L., The effects of gender, team size, and a shoulder harness on a stretcher-carry task and post-carry performance, Part I. A simulated carry from a remote site, Int Jour of Industrial Ergonomics, Vol 18, 1996, pp. 27 - 40.
[12] Dos Santos, M. L., Lockie, R. G., Orr, R., Dinyer-McNeely, T., Smith, D., McDonald, S., & Dawes, J. (2025). The Metabolic Demand of Firefighting: A Systematic Review. Physiologia, 5(2), 12.
[13] Jamnik, V.K., Thomas, S.G., Shaw, J.A., Gledhill, N., Identification and characterization of the critical physically demanding tasks encountered by correctional officers Applied Physiology, Nutrition, and Metabolism, No 35, Feb 2010, pp.45-58.
[14] Lavender, S., Conrad, K., Reichelt, P., Meyer, F., Johnson, P.. Postural analysis of paramedics simulating frequently performed strenuous tasks, Applied Ergonomics, Vol 31, 2000 pp. 45-57.
[15] Lewis-Schroeder, N. F., Kieran, K., Murphy, B. L., Wolff, J. D., Robinson, M. A., & Kaufman, M. L. (2018). Conceptualization, assessment, and treatment of traumatic stress in first responders: A review of critical issues. Harvard review of psychiatry, 26(4), 216-227.
[16] Syed, S., Ashwick, R., Schlosser, M., Jones, R., Rowe, S., & Billings, J. (2020). Global prevalence and risk factors for mental health problems in police personnel: a systematic review and meta-analysis. Occupational and environmental medicine, 77(11), 737-747.
[17] Spelten, E., van Vuuren, J., O’Meara, P., Thomas, B., Grenier, M., Ferron, R., & Agarwal, G. (2022). Workplace violence against emergency health care workers: What Strategies do Workers use?. BMC emergency medicine, 22(1), 78.
[18] Strömberg, A., Johansson, L., Leino, T., Lusa, S., Mankkinen, T., Pelastajien kokemukset Myyrmannin kauppakeskuksen pommiräjähdyksen pelastusoperaation aikana ja sen jälkeen - haastattelututkimus noin 1,5 vuotta tapahtuman jälkeen. Palosuojelurahaston rahoittama hanke, Työterveyslaitos, Helsinki, 2005.
[19] Cicognani, E., Pietrantoni, L., Palestini, L. & Prati, G., Emergency Workers Quality of Life: The Protective Role of Sense of Community, Efficacy Beliefs and Coping Strategies, Social Indicators Research, 2009. Available at: http://www.springerlink.com/content/h51r032g76558826
[20] Gallagher, S. & McGilloway, S., Living in critical times: The impact of critical incidents on frontline ambulance personnel--a qualitative perspective, International Journal of Emergency Mental Health, Vol. 9, No 3, 2007, pp. 215-223.
[21] ILO - International Labour Organization, Major Hazard Control – A practical guide, ILO, Geneva, Switzerland, 1988.
[22] FAII - Federation of Accident Insurance Institutions, Statistics, 2012. (personal communication)
[23] EU-OSHA - European Agency for Safety and Health at Work,. Emergency Services: A Literature Review on Occupational Safety and Health Risks, 2011, Available at: https://osha.europa.eu/en/publications/emergency-services-occupational-safety-and-health-risks
[24] Riihimäki, H., Overview. ILO, 2009. Available at: https://www.iloencyclopaedia.org/part-i-47946/musculoskeletal-system/item/271-overview
[25] ILO - International Labour Organization. International Hazard Datasheets on Occupation. Fire-fighter. Available at: https://www.ilo.org/publications/fire-fighter-international-hazard-datasheets-occupation
[26] ILO - International Labour Organization. International Hazard Datasheets on occupation. Police/Law Enforcement Officer. Available at: https://www.ilo.org/publications/officer-policelaw-enforcement-international-hazard-datasheets-occupation
[27] Wiitavaara, B., Lundman, B., Barnekow-Bergkvist, M., Brulin, C., Striking a balance - health experiences of male ambulance personnel with musculoskeletal symptoms: A grounded theory, International Journal of Nursing Studies Sweden, Vol. 44, 2007, pp. 770–779.
[28] Tahernejad, A., Makki, F., Rezaei, E., Marzban, H., Tahernejad, S., & Sahebi, A. (2024). Musculoskeletal disorders in emergency medical services personnel: a systematic review and meta-analysis. Public Health, 237, 107-115.
[29] Morren, M., Dirkzwager, A.J.E., Kessels, F.J.M., & Yzermans, C. J., The influence of a disaster on the health of rescue workers: a longitudinal study, Canadian Medical Association Journal, Vol. 176, No 9, 2005, pp. 1279-1283.
[30] Berríos-Torres, S.I., Greenko, J.A., Phillips, M., Miller, J.R., Treadwell, T.& Ikeda, R.M., World Trade Center rescue worker injury and illness surveillance, New York 2001, American Journal of Preventive Medicine, Vol. 25, No 2, 2003, pp. 79-87.
[31] United States, Department of Veterans Affairs, National Center for PTSD (2011). Disaster rescue and response workers.
[32] Jonsson, A., Segesten, K., & Mattsson, B., Post-traumatic stress among Swedish ambulance personnel, Emergency Medicine Journal, Vol. 20, 2003, pp. 79-84.
[33] Bennett, P., Williams, Y., Page, N., Hood, K., & Woollard, M., Levels of mental health problems among UK emergency ambulance workers, Emergency Medicine Journal, Vol. 21, 2004, pp. 235-236.
[34] IARC - International Agency for Research on Cancer. Volume 132: Occupational exposure as a firefighter. Available at: https://monographs.iarc.who.int/news-events/volume-132-occupational-exposure-as-a-firefighter/
[35] Sulsky, S.I., Birk, T., Cohen, L.C., Luippold, R.S., Heidenreich, M.J., & Nunes, A., Effectiveness of measures to prevent needlestick injuries among employees in health professions, Hauptverband der Gewerblichen Berufsgenossenschaften (HVBG), 2006.
[36] Rischitelli, G., Harris, J., McCauley, L., Gershon, R., & Guidotti, T., The risk of acquiring hepatitis B or C among public safety workers, American Journal of Preventive Medicine, Vol. 20, No 4, 2001, pp. 299-306.
[37] Ilmarinen, J., Towards a longer worklife! Ageing and the quality of worklife in the European Union, Finnish Institute of Occupational Health, Ministry of Social Affairs and Health, Helsinki, 2006.
[38] Tuomi, K., Ilmarinen, J., Eskelinen, L., Järvinen, E., Toikkanen, J., Klockars, M. Prevalence and incidence of diseases and work ability in different work categories of municipal occupations. Scand J Work Environ Health, 17 Suppl 1:67-74, 1991.
[39] Tuomi, K., Ilmarinen, J., Jahkola, A., Katajarinne, L., Tulkki, A., Work Ability Index. Occupational Health Care 19, Finnish Institute of Occupational Health, Helsinki, 1998.
[40] Ilmarinen, J. (2019). From work ability research to implementation. International journal of environmental research and public health, 16(16), 2882.
[41] Sörensen, L., Smolander, J., Louhevaara, V., Korhonen, O., Oja, P., Physical activity, fitness and body composition of Finnish police officers: a 15-year follow-up study, Occup med (Lond), Vol 50, 2000, pp. 3-10.
[42] Punakallio, A., Lusa, S., Luukkonen, R., Lindholm, H., Physical Capacities for Predicting the Perceived Work Ability of Firefighters. In: Nygård C-H, Savinainen M, Kirsi T and Lumme-Sandt K eds. Age Management during the Life Course. Proceedings of the 4th Symposium on Work Ability, Tampere, Finland, June 6-9 2010, Tampere University Press, Tampere, 2011; pp. 150-160.
[43] Ilmarinen, J., Tuomi, K., Klockars, M., Changes in the work ability of active employees over an 11-year period0146. Scand J work Environ Health, Vol 23, suppl 1, 1997, pp 49-57.
[44] Lusa, S., Punakallio, A., Luukkonen, R., Factors Predicting Perceived Work Ability of Finnish Firefighters, In: Nygård C-H, Savinainen M, Kirsi T and Lumme-Sandt K eds. Age Management during the Life Course. Proceedings of the 4th Symposium on Work Ability, Tampere, Finland, June 6-9 2010. Tampere University Press, Tampere, 2011, pp. 161-169.
[45] Pokorski, J., Niteck, J., Ilmarinen, J.,: Work ability index in fire fighters and medical doctors. In: Ilmarinen J, Lehtinen S, eds. Past, present and future of work ability. People and Work Research Reports 65. Finnish Institute of Occupational Health Helsinki, 2004, pp. 106-13.
[46] Eurostat Newsrelease, Active ageing in the EU, Publications Office of the European Union, Luxembourg, 2012.
[47] Eurostat. Database: Population on 1 January by age group and sex (demo_pjangroup). Available at: https://ec.europa.eu/eurostat/web/main/data/database
[48] Eurostat. Statistics explained: Population structure and ageing. Available at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing
[49] Sluiter, J.K., High-demand jobs: Age-related diversity in work ability? Applied Ergonomics, Vol. 37, 2006, pp 429-440.
[50] Sehl, M.E., Yates, F.E., 2001. Kinetics of human aging. I: rates of senescence between ages 30 and 70 years in healthy people. J. Gerontol. Vol 56A, pp. B198-B208.
[51] Jackson, B.A., Baker, J.C., Ridgely, M.S., Bartis, J.T., & Linn, H.I., Protecting Emergency Responders. Volume 3 Safety Management in disaster and terrorism response. Cincinnati: Centres for Disease Control and Prevention National Institute for Occupational Safety and Health. Department of Health and Human Services, 2004.
[52] Jackson, B.A., Peterson, T.J, Bartis, J.T., LaTourrette, T., Brahmakulam, I.T., Houser, A., & Sollinger, J.M., Protecting emergency responders: Lessons learned from terrorist attacks. RAND, Santa Monica - Arlington - Pittsburgh, 2002.
[53] Gabriel, R., Ferrando, L., Cortón, E.S., Mingote, C., García-Camba, E., Liria, A.F., & Galea, S, Psychopathological consequences after a terrorist attack: An epidemiological study among victims, the general population, and police officers, European Psychiatry, Vol. 22, Issue 6, 2007, pp. 339-346.
[54] Perrin, M. A.., DiGrande, L., Wheeler, K., Thorpe, L., Farfel, M., & Brackbill, R., Differences in PTSD Prevalence and Associated Risk Factors Among World Trade Center Disaster Rescue and Recovery Workers, American Journal of Psychiatry, Vol. 164, 2007, pp. 1385-1394.
[55] Oikeusministeriö (Ministry of Justice, Finland), Jokelan koulusurmat 7.11.2007 Tutkijalautakunnan raportti, Julkaisu 2009:2. The school shootings of Jokela 7.11.2007. Report of the Court of Inquiry.
EU-OSHA - European Agency for Safety and Health at Work, Emergency Services: A Literature Review on Occupational Safety and Health Risks, Publications Office of the European Union, Luxembourg, 2011. Available at: https://osha.europa.eu/en/publications/emergency-services-occupational-safety-and-health-risks
Odabir teme